

Two new cases of anti-Ca (anti-ARHGAP26/GRAF) autoantibody-associated cerebellar ataxia
- PMID: 23320754
- PMCID: PMC3549891
- DOI: 10.1186/1742-2094-10-7
Two new cases of anti-Ca (anti-ARHGAP26/GRAF) autoantibody-associated cerebellar ataxia
Abstract
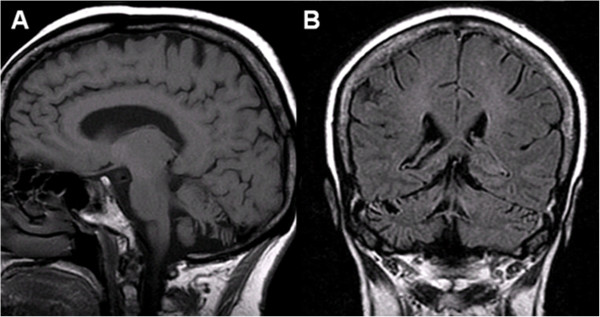
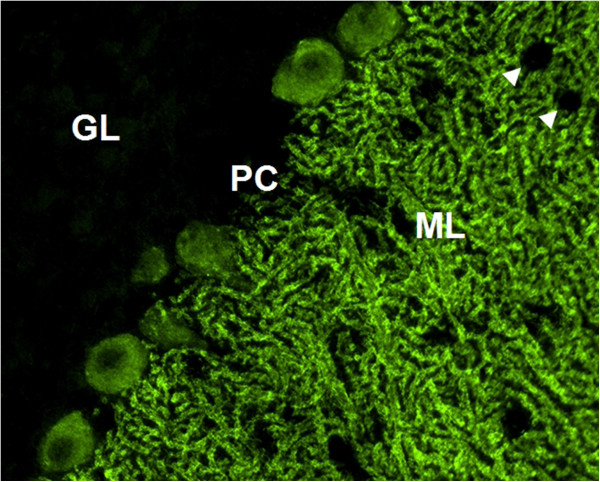
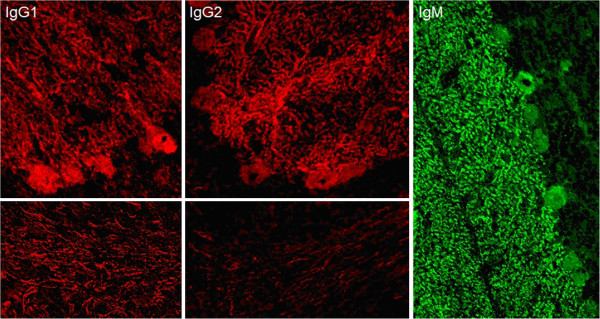
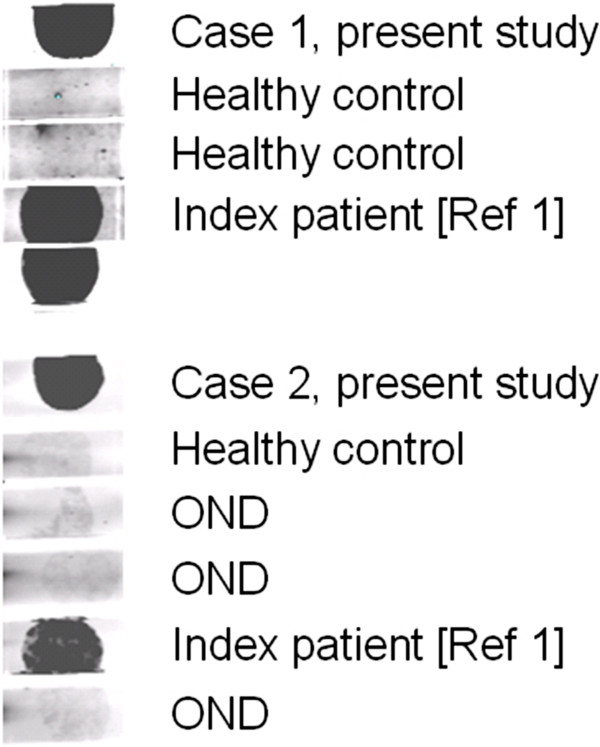
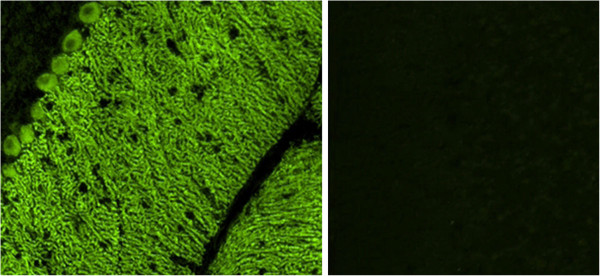
Recently, we discovered a novel serum and cerebrospinal fluid (CSF) autoantibody (anti-Ca) to Purkinje cells in a patient with autoimmune cerebellar ataxia (ACA) and identified the RhoGTPase-activating protein 26 (ARHGAP26; alternative designations include GTPase regulator associated with focal adhesion kinase pp125, GRAF, and oligophrenin-1-like protein, OPHN1L) as the target antigen. Here, we report on two new cases of ARHGAP26 autoantibody-positive ACA that were first diagnosed after publication of the index case study. While the index patient developed ACA following an episode of respiratory infection with still no evidence for malignancy 52 months after onset, neurological symptoms heralded ovarian cancer in one of the patients described here. Our finding of anti-Ca/anti-ARHGAP26 antibodies in two additional patients supports a role of autoimmunity against ARHGAP26 in the pathogenesis of ACA. Moreover, the finding of ovarian cancer in one of our patients suggests that anti-Ca/anti-ARHGAP26-positive ACA might be of paraneoplastic aetiology in some cases. In conclusion, testing for anti-Ca/anti-ARHGAP26 should be included in the diagnostic work-up of patients with ACA, and an underlying tumour should be considered in patients presenting with anti-Ca/ARHGAP26 antibody-positive ACA.
Figures
References
-
- Graus F, Delattre JY, Antoine JC, Dalmau J, Giometto B, Grisold W, Honnorat J, Smitt PS, Vedeler C, Verschuuren JJ, Vincent A, Voltz R. Recommended diagnostic criteria for paraneoplastic neurological syndromes. J Neurol Neurosurg Psychiatry. 2004;75:1135–1140. doi: 10.1136/jnnp.2003.034447. - DOI - PMC - PubMed
-
- Uhlen M, Bjorling E, Agaton C, Szigyarto CA, Amini B, Andersen E, Andersson AC, Angelidou P, Asplund A, Asplund C, Berglund L, Bergstrom K, Brumer H, Cerjan D, Ekstrom M, Elobeid A, Eriksson C, Fagerberg L, Falk R, Fall J, Forsberg M, Bjorklund MG, Gumbel K, Halimi A, Hallin I, Hamsten C, Hansson M, Hedhammar M, Hercules G, Kampf C. et al. A human protein atlas for normal and cancer tissues based on antibody proteomics. Mol Cell Proteomics. 2005;4:1920–1932. doi: 10.1074/mcp.M500279-MCP200. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
