

Dietary fortificant iron intake is negatively associated with quality of life in patients with mildly active inflammatory bowel disease
- PMID: 23320878
- PMCID: PMC3568053
- DOI: 10.1186/1743-7075-10-9
Dietary fortificant iron intake is negatively associated with quality of life in patients with mildly active inflammatory bowel disease
Abstract
Background: Iron deficiency anaemia and oral iron supplementation have been associated negatively with quality of life, and with adverse effects, respectively, in subjects with inflammatory bowel disease (IBD). Hence, the risk-benefit ratio of oral iron is not understood in this patient group. The present case-control study investigated whether dietary iron intake impacts on quality of life in IBD patients.
Methods: Quality of life, habitual dietary iron intakes and iron requirements were assessed in 29 patients with inactive or mildly active IBD as well as in 28 healthy control subjects.
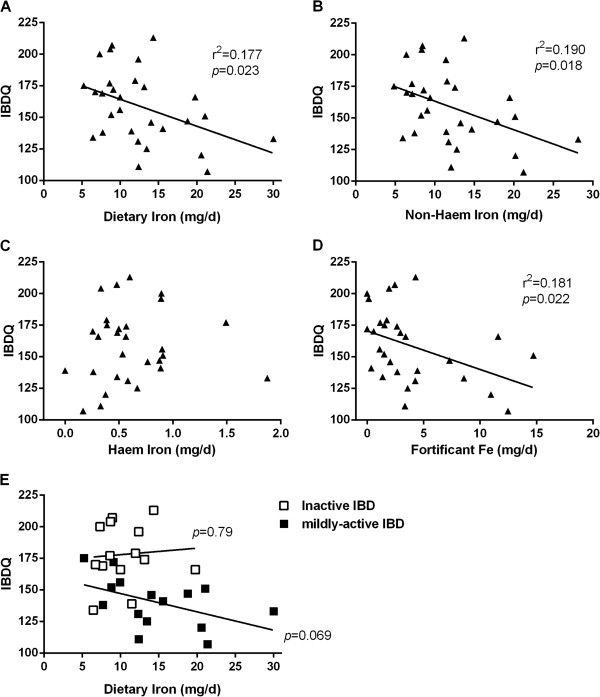
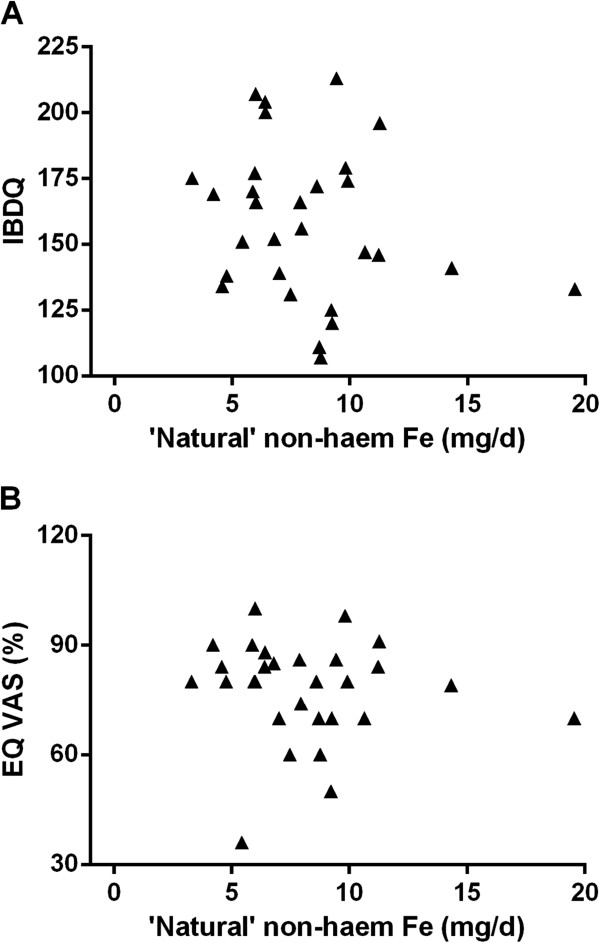
Results: As expected, quality of life was worse in IBD patients as a whole in comparison to healthy controls according to EuroQol score and EuroQol VAS percentage (6.9 ± 1.6 vs 5.3 ± 0.6; p< 0.0001 and 77 ± 14% vs 88 ± 12%; p=0.004 respectively). For IBD subjects, 21/29 were iron deplete based upon serum iron responses to oral iron but, overall, were non-anaemic with mean haemoglobin of 13.3 ± 1.5 g/dL, and there was no difference in their quality of life compared to 8/29 iron replete subjects (Hb 14.0 ± 0.8 g/dL). Interestingly, total dietary iron intake was significantly negatively associated with quality of life in IBD patients, specifically for non-haem iron and, more specifically, for fortificant iron. Moreover, for total non-haem iron the negative association disappeared when fortificant iron values were subtracted. Finally, further sub-analysis indicated that the negative association between (fortificant) dietary iron intake and quality of life in IBD patients is driven by findings in patients with mildly active disease rather than in patients with quiescent disease.
Conclusions: Iron deficiency per se (i.e. without concomitant anaemia) does not appear to further affect quality of life in IBD patients with inactive or mildly active disease. However, in this preliminary study, dietary iron intake, particularly fortificant iron, appears to be significantly negatively associated with quality of life in patients with mildly active disease.
Figures

Similar articles
-
Dietary iron does not impact the quality of life of patients with quiescent ulcerative colitis: an observational study.Nutr J. 2013 Nov 23;12:152. doi: 10.1186/1475-2891-12-152. Nutr J. 2013. PMID: 24267915 Free PMC article.
-
Iron status is inversely associated with dietary iron intakes in patients with inactive or mildly active inflammatory bowel disease.Nutr Metab (Lond). 2013 Feb 1;10(1):18. doi: 10.1186/1743-7075-10-18. Nutr Metab (Lond). 2013. PMID: 23374396 Free PMC article.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Iron requirements based upon iron absorption tests are poorly predicted by haematological indices in patients with inactive inflammatory bowel disease.Br J Nutr. 2012 Jun;107(12):1806-11. doi: 10.1017/S0007114511004971. Epub 2011 Dec 9. Br J Nutr. 2012. PMID: 22152498 Free PMC article.
-
Fatigue and acute/chronic anaemia.Dan Med J. 2014 Apr;61(4):B4824. Dan Med J. 2014. PMID: 24814598 Review.
Cited by
-
Iron Treatment May Be Difficult in Inflammatory Diseases: Inflammatory Bowel Disease as a Paradigm.Nutrients. 2018 Dec 11;10(12):1959. doi: 10.3390/nu10121959. Nutrients. 2018. PMID: 30544934 Free PMC article. Review.
-
The Correlation Between MYO9B Gene Polymorphism and Inflammatory Bowel Disease in the Guangxi Zhuang Population.Int J Gen Med. 2021 Dec 1;14:9163-9172. doi: 10.2147/IJGM.S338142. eCollection 2021. Int J Gen Med. 2021. PMID: 34880655 Free PMC article.
-
Dietary iron does not impact the quality of life of patients with quiescent ulcerative colitis: an observational study.Nutr J. 2013 Nov 23;12:152. doi: 10.1186/1475-2891-12-152. Nutr J. 2013. PMID: 24267915 Free PMC article.
-
Hepcidin expression in colon during trinitrobenzene sulfonic acid-induced colitis in rats.World J Gastroenterol. 2014 Apr 21;20(15):4345-52. doi: 10.3748/wjg.v20.i15.4345. World J Gastroenterol. 2014. PMID: 24764672 Free PMC article.
-
Exploring progress in iron supplement formulation approaches for treating iron deficiency anemia through bibliometric and thematic analysis.Heliyon. 2024 Apr 4;10(7):e29058. doi: 10.1016/j.heliyon.2024.e29058. eCollection 2024 Apr 15. Heliyon. 2024. PMID: 38623202 Free PMC article. Review.
References
-
- Gasche C, Dejaco C, Waldhoer T, Tillinger W, Reinisch W, Fueger GF, Gangl A, Lochs H. Intravenous iron and erythropoietin for anemia associated with Crohn disease. A randomized, controlled trial. Ann Intern Med. 1997;126:782–787. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
