

Impact of the human immunodeficiency virus on early multidrug-resistant tuberculosis treatment outcomes in Botswana
- PMID: 23321297
- PMCID: PMC4393740
- DOI: 10.5588/ijtld.12.0100
Impact of the human immunodeficiency virus on early multidrug-resistant tuberculosis treatment outcomes in Botswana
Abstract
Setting: The impact of the human immunodeficiency virus (HIV) on multidrug-resistant tuberculosis (MDR-TB) treatment outcomes in sub-Saharan Africa, where extensive rollout of highly active antiretroviral therapy (HAART) has occurred, remains unclear.
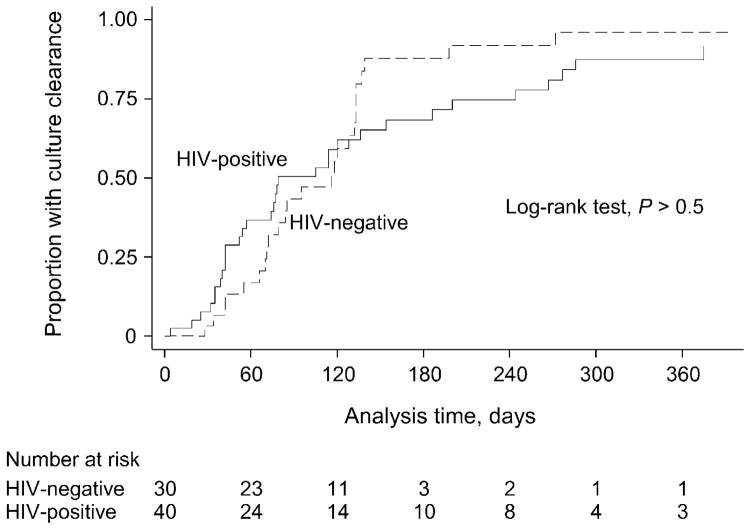
Objective: To compare the time to initial culture conversion among patients with and those without HIV infection in a setting of individualized MDR-TB care in Botswana.
Design: Prospective cohort study of MDR-TB patients receiving ambulatory, integrated TB-HIV care at two public clinics in Botswana. The time to culture conversion was compared by HIV status using Cox proportional hazard ratios (HRs).
Results: A total of 40 HIV-infected and 30 non-HIV-infected patients with MDR-TB and follow-up cultures were identified. The median time to initial culture conversion was 78 days (interquartile range [IQR] 42-186) for HIV-infected and 95 days (IQR 70-133) for non-HIV-infected individuals (log rank P > 0.5; unadjusted HR 0.9, 95%CI 0.5-1.5). Adjusting for age, sex, treatment history and number of active anti-tuberculosis drugs did not change this result (adjusted HR 0.8, 95%CI 0.4-1.4).
Conclusion: We found no difference in the proportion of or time to initial sputum culture conversion between an HIV-infected and a non-infected cohort of MDR-TB patients in Botswana, suggesting that outcomes may be comparable in similar settings with access to individualized anti-tuberculosis treatment and HAART.
Conflict of interest statement
Conflict of interest: none declared.
Figures
References
-
- Maartens G, Wilkinson RJ. Tuberculosis. Lancet. 2007;370:2030–2043. - PubMed
-
- Mukherjee JS, Rich ML, Socci AR, et al. Programmes and principles in treatment of multidrug-resistant tuberculosis. Lancet. 2004;363:474–481. - PubMed
-
- Orenstein EW, Basu S, Shah NS, et al. Treatment outcomes among patients with multidrug-resistant tuberculosis: systematic review and meta-analysis. Lancet Infect Dis. 2009;9:153–161. - PubMed
-
- Goble M, Iseman MD, Madsen LA, Waite D, Ackerson L, Horsburgh CR., Jr Treatment of 171 patients with pulmonary tuberculosis resistant to isoniazid and rifampin. N Engl J Med. 1993;328:527–532. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
