

All-cause mortality in 272,186 patients hospitalized with incident atrial fibrillation 1995-2008: a Swedish nationwide long-term case-control study
- PMID: 23321349
- PMCID: PMC3618889
- DOI: 10.1093/eurheartj/ehs469
All-cause mortality in 272,186 patients hospitalized with incident atrial fibrillation 1995-2008: a Swedish nationwide long-term case-control study
Abstract
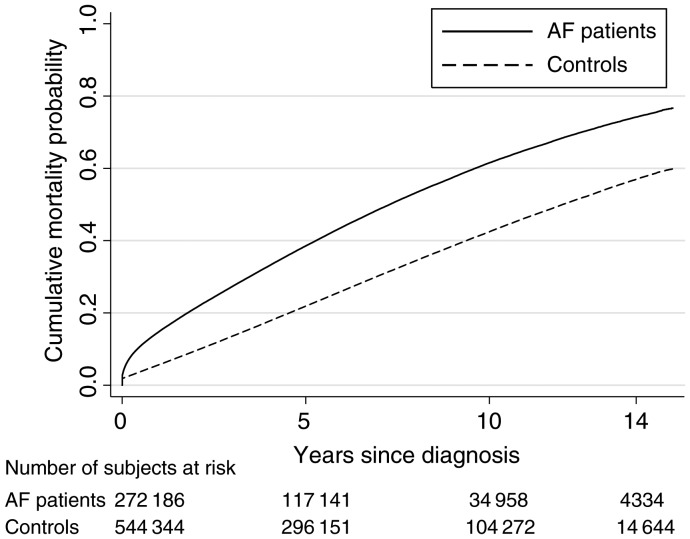
Aims: To evaluate long-term all-cause risk of mortality in women and men hospitalized for the first time with atrial fibrillation (AF) compared with matched controls.
Methods and results: A total of 272 186 patients (44% women) ≤ 85 years at the time of hospitalization with incidental AF 1995-2008 and 544 344 matched controls free of in-hospital diagnosis of AF were identified. Patients were followed via record linkage of the Swedish National Patient Registry and the Cause of Death Registry. Using Cox regression models, the long-term relative all-cause mortality risk, adjusted for concomitant diseases, in women vs. controls was 2.15, 1.72, and 1.44 (P < 0.001) in the age categories ≤ 65, 65-74, and 75-85 years, respectively. The corresponding figures for men were 1.76, 1.36, and 1.24 (P < 0.001). Among concomitant diseases, neoplasm, chronic renal failure, and chronic obstructive pulmonary disease contributed most to the increased all-cause mortality vs. controls. In patients with AF as the primary diagnosis, the relative risk of mortality was 1.63, 1.46, and 1.28 (P < 0.001) in women and 1.45, 1.17, and 1.10 (P < 0.001) in men.
Conclusion: Atrial fibrillation was an independent risk factor of all-cause mortality in patients with incident AF. The concomitant diseases that contributed most were found outside the thromboembolic risk scores. The highest relative risk of mortality was seen in women and in the youngest patients compared with controls, and the differences between genders in each age category were statistically significant.
Figures
Comment in
-
Atrial fibrillation is associated with increased mortality: causation or association?Eur Heart J. 2013 Apr;34(14):1027-30. doi: 10.1093/eurheartj/eht044. Epub 2013 Feb 13. Eur Heart J. 2013. PMID: 23407094 No abstract available.
References
-
- Miyasaka Y, Barnes ME, Gersh BJ, Cha SS, Bailey KR, Abhayaratna WP, Seward JB, Tsang TS. Secular trends in incidence of atrial fibrillation in Olmstead County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation. 2006;114:119–125. doi:10.1161/CIRCULATIONAHA.105.595140. - DOI - PubMed
-
- Heeringa J, van der Kuip DA, Hofman A, Kors JA, van Herpen G, Stricker BH, Stijnen T, Lip GY, Witteman JC. Prevalence, incidence and lifetime risk of atrial fibrillation: the Rotterdam study. Eur Heart J. 2006;27:949–953. doi:10.1093/eurheartj/ehi825. - DOI - PubMed
-
- Frost L, Vestergaard P, Mosekilde L, Mortensen LS. Trends in incidence and mortality in the hospital diagnosis of atrial fibrillation or flutter in Denmark, 1980–1999. Int J Cardiol. 2005;103:78–84. doi:10.1016/j.ijcard.2004.08.024. - DOI - PubMed
-
- Wolf PA, Mitchell JB, Baker CS, Kannel WB, D'Agostino RB. Impact of atrial fibrillation on mortality, stroke, and medical costs. Arch Intern Med. 1998;158:229–234. doi:10.1001/archinte.158.3.229. - DOI - PubMed
-
- Wachtell K, Hornestam B, Lehto M, Slotwiner DJ, Gerdts E, Olsen MH, Aurup P, Dahlöf B, Ibsen H, Julius S, Kjeldsen SE, Lindholm LH, Nieminen MS, Rokkedal J, Devereux RB. Cardiovascular morbidity and mortality in hypertensive patients with a history of atrial fibrillation: the Losartan Intervention for End point Reduction in Hypertension (LIFE) study. J Am Coll Cardiol. 2005;45:705–711. doi:10.1016/j.jacc.2004.06.080. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
