

Accuracy of CT cerebral perfusion in predicting infarct in the emergency department: lesion characterization on CT perfusion based on commercially available software
- PMID: 23322329
- PMCID: PMC3661911
- DOI: 10.1007/s10140-012-1102-8
Accuracy of CT cerebral perfusion in predicting infarct in the emergency department: lesion characterization on CT perfusion based on commercially available software
Abstract
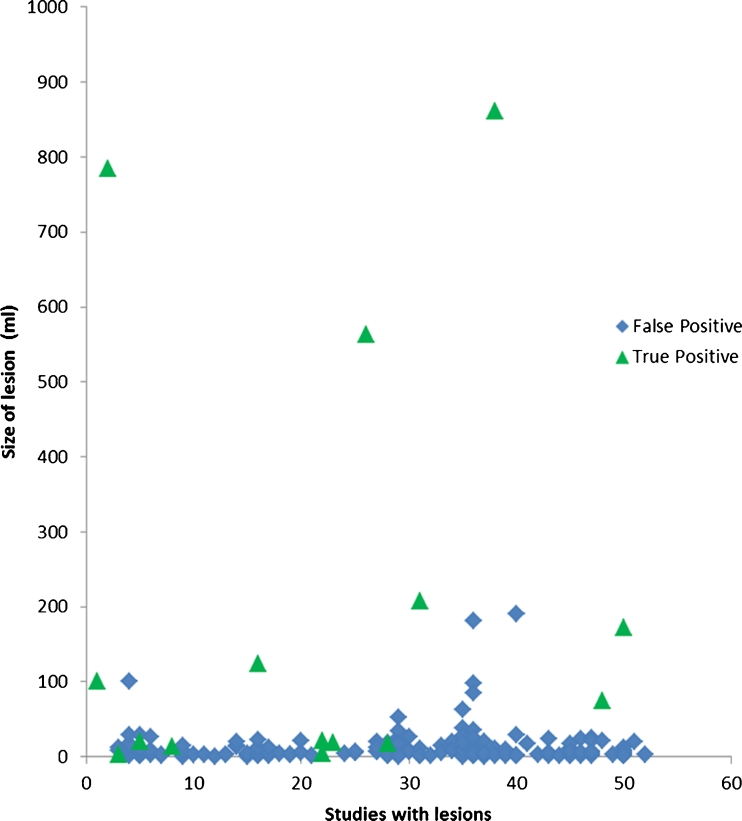
This study aims to assess the diagnostic accuracy of a single vendor commercially available CT perfusion (CTP) software in predicting stroke. A retrospective analysis on patients presenting with stroke-like symptoms within 6 h with CTP and diffusion-weighted imaging (DWI) was performed. Lesion maps, which overlays areas of computer-detected abnormally elevated mean transit time (MTT) and decreased cerebral blood volume (CBV), were assessed from a commercially available software package and compared to qualitative interpretation of color maps. Using DWI as the gold standard, parameters of diagnostic accuracy were calculated. Point biserial correlation was performed to assess for relationship of lesion size to a true positive result. Sixty-five patients (41 females and 24 males, age range 22-92 years, mean 57) were included in the study. Twenty-two (34 %) had infarcts on DWI. Sensitivity (83 vs. 70 %), specificity (21 vs. 69 %), negative predictive value (77 vs. 84 %), and positive predictive value (29 vs. 50 %) for lesion maps were contrasted to qualitative interpretation of perfusion color maps, respectively. By using the lesion maps to exclude lesions detected qualitatively on color maps, specificity improved (80 %). Point biserial correlation for computer-generated lesions (R pb = 0.46, p < 0.0001) and lesions detected qualitatively (R pb = 0.32, p = 0.0016) demonstrated positive correlation between size and infarction. Seventy-three percent (p = 0.018) of lesions which demonstrated an increasing size from CBV, cerebral blood flow, to MTT/time to peak were true positive. Used in isolation, computer-generated lesion maps in CTP provide limited diagnostic utility in predicting infarct, due to their inherently low specificity. However, when used in conjunction with qualitative perfusion color map assessment, the lesion maps can help improve specificity.
Figures





References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
