

Urban tree canopy and asthma, wheeze, rhinitis, and allergic sensitization to tree pollen in a New York City birth cohort
- PMID: 23322788
- PMCID: PMC3620770
- DOI: 10.1289/ehp.1205513
Urban tree canopy and asthma, wheeze, rhinitis, and allergic sensitization to tree pollen in a New York City birth cohort
Abstract
Background: Urban landscape elements, particularly trees, have the potential to affect airflow, air quality, and production of aeroallergens. Several large-scale urban tree planting projects have sought to promote respiratory health, yet evidence linking tree cover to human health is limited.
Objectives: We sought to investigate the association of tree canopy cover with subsequent development of childhood asthma, wheeze, rhinitis, and allergic sensitization.
Methods: Birth cohort study data were linked to detailed geographic information systems data characterizing 2001 tree canopy coverage based on LiDAR (light detection and ranging) and multispectral imagery within 0.25 km of the prenatal address. A total of 549 Dominican or African-American children born in 1998-2006 had outcome data assessed by validated questionnaire or based on IgE antibody response to specific allergens, including a tree pollen mix.
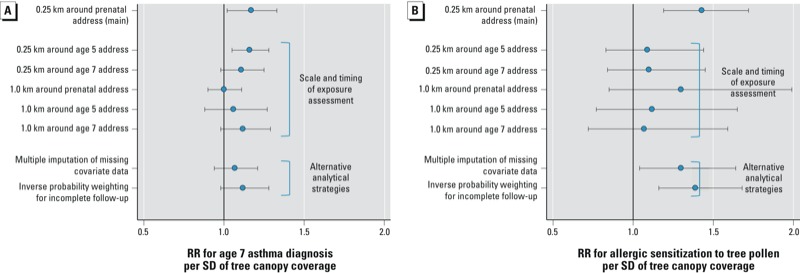
Results: Tree canopy coverage did not significantly predict outcomes at 5 years of age, but was positively associated with asthma and allergic sensitization at 7 years. Adjusted risk ratios (RRs) per standard deviation of tree canopy coverage were 1.17 for asthma (95% CI: 1.02, 1.33), 1.20 for any specific allergic sensitization (95% CI: 1.05, 1.37), and 1.43 for tree pollen allergic sensitization (95% CI: 1.19, 1.72).
Conclusions: Results did not support the hypothesized protective association of urban tree canopy coverage with asthma or allergy-related outcomes. Tree canopy cover near the prenatal address was associated with higher prevalence of allergic sensitization to tree pollen. Information was not available on sensitization to specific tree species or individual pollen exposures, and results may not be generalizable to other populations or geographic areas.
Conflict of interest statement
The sponsors had no role in the design, conduct, or publication of the research. The authors retained full control of all the data.
The authors declare they have no actual or potential competing financial interests.
Figures

Similar articles
-
Sensitization to common allergens and its association with allergic disorders at age 4 years: a whole population birth cohort study.Pediatrics. 2001 Aug;108(2):E33. doi: 10.1542/peds.108.2.e33. Pediatrics. 2001. PMID: 11483843
-
Early predictors for developing allergic disease and asthma: examining separate steps in the 'allergic march'.Clin Exp Allergy. 2007 Sep;37(9):1296-302. doi: 10.1111/j.1365-2222.2007.02796.x. Clin Exp Allergy. 2007. PMID: 17845409
-
Comparative degree and type of sensitization to common indoor and outdoor allergens in subjects with allergic rhinitis and/or asthma.Clin Exp Allergy. 1997 Jan;27(1):52-9. Clin Exp Allergy. 1997. PMID: 9117881
-
Climate Change and the Future of Allergies and Asthma.Curr Allergy Asthma Rep. 2025 Mar 27;25(1):20. doi: 10.1007/s11882-025-01201-0. Curr Allergy Asthma Rep. 2025. PMID: 40146339 Review.
-
Climate Change and Allergens: Current and Future Impacts.J Allergy Clin Immunol Pract. 2025 Jun;13(6):1281-1288. doi: 10.1016/j.jaip.2025.02.039. Epub 2025 Mar 10. J Allergy Clin Immunol Pract. 2025. PMID: 40074172 Review.
Cited by
-
Allergenic pollen production across a large city for common ragweed (Ambrosia artemisiifolia).Landsc Urban Plan. 2019 Oct;190:103615. doi: 10.1016/j.landurbplan.2019.103615. Epub 2019 Jul 20. Landsc Urban Plan. 2019. PMID: 32831442 Free PMC article.
-
A systematic review of associations between environmental exposures and development of asthma in children aged up to 9 years.BMJ Open. 2014 Nov 24;4(11):e006554. doi: 10.1136/bmjopen-2014-006554. BMJ Open. 2014. PMID: 25421340 Free PMC article.
-
Approaching environmental health disparities and green spaces: an ecosystem services perspective.Int J Environ Res Public Health. 2015 Feb 10;12(2):1952-68. doi: 10.3390/ijerph120201952. Int J Environ Res Public Health. 2015. PMID: 25674782 Free PMC article.
-
Association between Asthma Control and Exposure to Greenness and Other Outdoor and Indoor Environmental Factors: A Longitudinal Study on a Cohort of Asthmatic Children.Int J Environ Res Public Health. 2022 Jan 4;19(1):512. doi: 10.3390/ijerph19010512. Int J Environ Res Public Health. 2022. PMID: 35010773 Free PMC article.
-
Short term physician visits and medication prescriptions for allergic disease associated with seasonal tree, grass, and weed pollen exposure across the United States.Environ Health. 2021 Jul 21;20(1):85. doi: 10.1186/s12940-021-00766-3. Environ Health. 2021. PMID: 34289856 Free PMC article.
References
-
- Akinbami LJ, Schoendorf KC. Trends in childhood asthma: prevalence, health care utilization, and mortality. Pediatrics. 2002;110:315–322. - PubMed
-
- Arshad SH, Matthews S, Gant C, Hide DW. Effect of allergen avoidance on development of allergic disorders in infancy. Lancet. 1992;339:1493–1497. - PubMed
-
- Asero R. Birch and ragweed pollinosis north of Milan: a model to investigate the effects of exposure to “new” airborne allergens. Allergy. 2002;57:1063–1066. - PubMed
-
- Asero R. Analysis of new respiratory allergies in patients monosensitized to airborne allergens in the area north of Milan. J Investig Allergol Clin Immunol. 2004;14:208–213. - PubMed
-
- Bealey WJ, McDonald AG, Nemitz E, Donovan R, Dragosits U, Duffy TR, et al. Estimating the reduction of urban PM10 concentrations by trees within an environmental information system for planners. J Environ Manag. 2007;85:44–58. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- RR00645/RR/NCRR NIH HHS/United States
- R01 ES012468/ES/NIEHS NIH HHS/United States
- R01 ES010165/ES/NIEHS NIH HHS/United States
- R01 ES008977/ES/NIEHS NIH HHS/United States
- R01ES014393/ES/NIEHS NIH HHS/United States
- 5R01ES008977/ES/NIEHS NIH HHS/United States
- 5P01ES009600/ES/NIEHS NIH HHS/United States
- P30 ES009089/ES/NIEHS NIH HHS/United States
- 5R01ES012468/ES/NIEHS NIH HHS/United States
- P01 ES009600/ES/NIEHS NIH HHS/United States
- M01 RR000645/RR/NCRR NIH HHS/United States
- K01HD067390/HD/NICHD NIH HHS/United States
- 5R01ES11158/ES/NIEHS NIH HHS/United States
- RD-832141/RD/ORD VA/United States
- R01 ES011158/ES/NIEHS NIH HHS/United States
- R01ES13163/ES/NIEHS NIH HHS/United States
- R01 ES014393/ES/NIEHS NIH HHS/United States
- 5R01ES10165/ES/NIEHS NIH HHS/United States
- P30ES009089/ES/NIEHS NIH HHS/United States
- K01 HD067390/HD/NICHD NIH HHS/United States
- R01 ES013163/ES/NIEHS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
