

Effectiveness of late gadolinium enhancement to improve outcomes prediction in patients referred for cardiovascular magnetic resonance after echocardiography
- PMID: 23324403
- PMCID: PMC3599652
- DOI: 10.1186/1532-429X-15-6
Effectiveness of late gadolinium enhancement to improve outcomes prediction in patients referred for cardiovascular magnetic resonance after echocardiography
Abstract
Background: Echocardiography (echo) is a first line test to assess cardiac structure and function. It is not known if cardiovascular magnetic resonance (CMR) with late gadolinium enhancement (LGE) ordered during routine clinical practice in selected patients can add additional prognostic information after routine echo. We assessed whether CMR improves outcomes prediction after contemporaneous echo, which may have implications for efforts to optimize processes of care, assess effectiveness, and allocate limited health care resources.
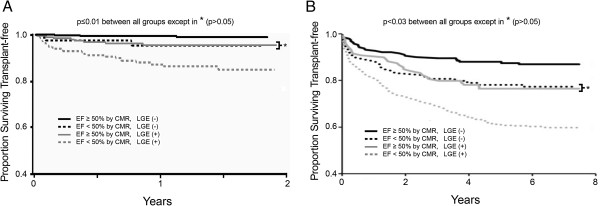
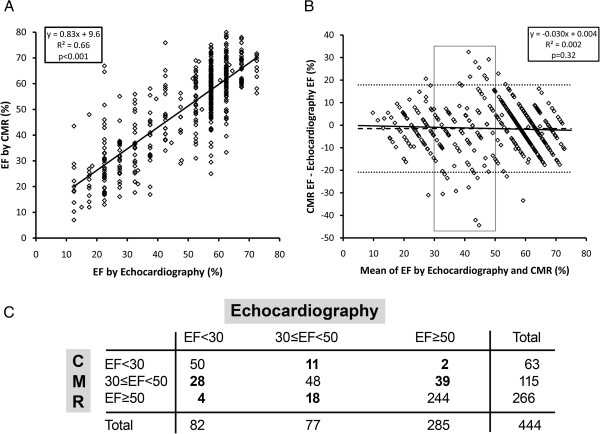
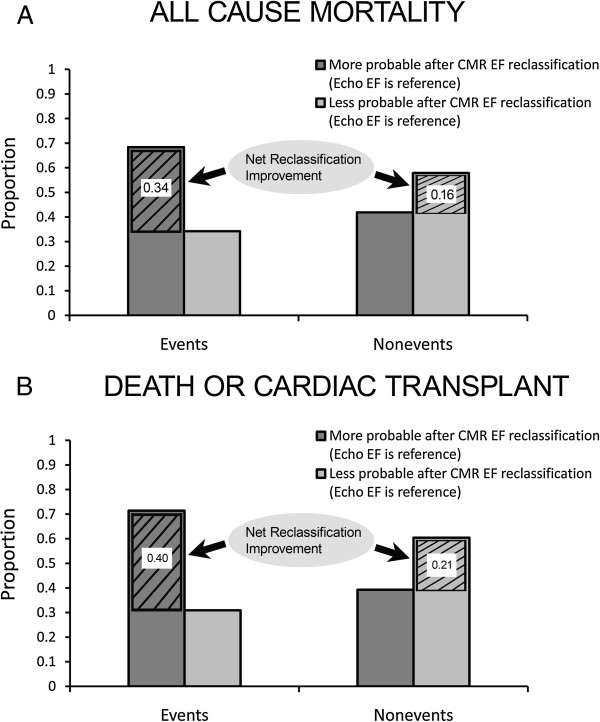
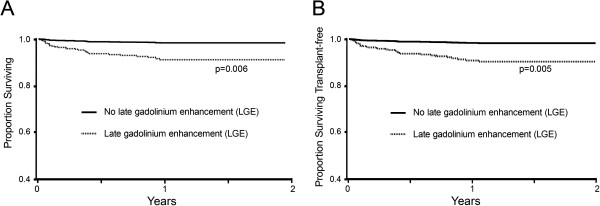
Methods and results: We prospectively enrolled 1044 consecutive patients referred for CMR. There were 38 deaths and 3 cardiac transplants over a median follow-up of 1.0 years (IQR 0.4-1.5). We first reproduced previous survival curve strata (presence of LGE and ejection fraction (EF) < 50%) for transplant free survival, to support generalizability of any findings. Then, in a subset (n = 444) with contemporaneous echo (median 3 days apart, IQR 1-9), EF by echo (assessed visually) or CMR were modestly correlated (R(2) = 0.66, p < 0.001), and 30 deaths and 3 transplants occurred over a median follow-up of 0.83 years (IQR 0.29-1.40). CMR EF predicted mortality better than echo EF in univariable Cox models (Integrated Discrimination Improvement (IDI) 0.018, 95% CI 0.008-0.034; Net Reclassification Improvement (NRI) 0.51, 95% CI 0.11-0.85). Finally, LGE further improved prediction beyond EF as determined by hazard ratios, NRI, and IDI in all Cox models predicting mortality or transplant free survival, adjusting for age, gender, wall motion, and EF.
Conclusions: Among those referred for CMR after echocardiography, CMR with LGE further improves risk stratification of individuals at risk for death or death/cardiac transplant.
Figures
References
-
- Chuang ML, Hibberd MG, Salton CJ, Beaudin RA, Riley MF, Parker RA, Douglas PS, Manning WJ. Importance of imaging method over imaging modality in noninvasive determination of left ventricular volumes and ejection fraction: assessment by two- and three-dimensional echocardiography and magnetic resonance imaging. J Am Coll Cardiol. 2000;35:477–484. doi: 10.1016/S0735-1097(99)00551-3. - DOI - PubMed
-
- Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, Picard MH, Roman MJ, Seward J, Shanewise JS. et al.Recommendations for chamber quantification: a report from the american society of Echocardiography's guidelines and standards committee and the chamber quantification writing group, developed in conjunction with the european association of echocardiography, a branch of the european society of cardiology. J Am Soc Echocardiogr. 2005;18:1440–1463. doi: 10.1016/j.echo.2005.10.005. - DOI - PubMed
-
- Caiani EG, Corsi C, Zamorano J, Sugeng L, MacEneaney P, Weinert L, Battani R, Gutierrez-Chico JL, Koch R, Perez de Isla L. et al.Improved semiautomated quantification of left ventricular volumes and ejection fraction using 3-dimensional echocardiography with a full matrix-array transducer: comparison with magnetic resonance imaging. J Am Soc Echocardiogr. 2005;18:779–788. doi: 10.1016/j.echo.2004.12.015. - DOI - PubMed
-
- Cicala S, de Simone G, Roman MJ, Best LG, Lee ET, Wang W, Welty TK, Galloway JM, Howard BV, Devereux RB. Prevalence and prognostic significance of wall-motion abnormalities in adults without clinically recognized cardiovascular disease: the strong heart study. Circulation. 2007;116:143–150. doi: 10.1161/CIRCULATIONAHA.106.652149. - DOI - PubMed
-
- Cheong BY, Muthupillai R, Wilson JM, Sung A, Huber S, Amin S, Elayda MA, Lee VV, Flamm SD. Prognostic significance of delayed-enhancement magnetic resonance imaging: survival of 857 patients with and without left ventricular dysfunction. Circulation. 2009;120:2069–2076. doi: 10.1161/CIRCULATIONAHA.109.852517. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
