

Grey matter damage in multiple sclerosis: a pathology perspective
- PMID: 23324595
- PMCID: PMC3609053
- DOI: 10.4161/pri.23499
Grey matter damage in multiple sclerosis: a pathology perspective
Abstract
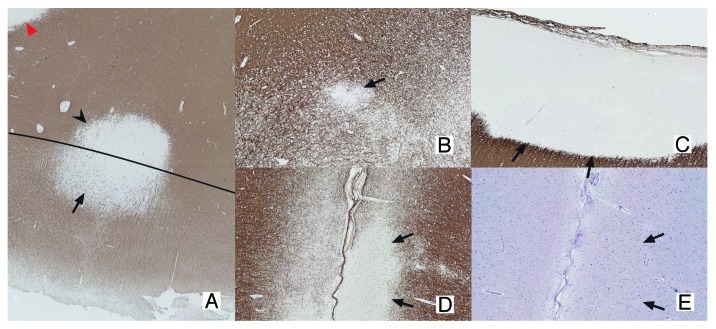
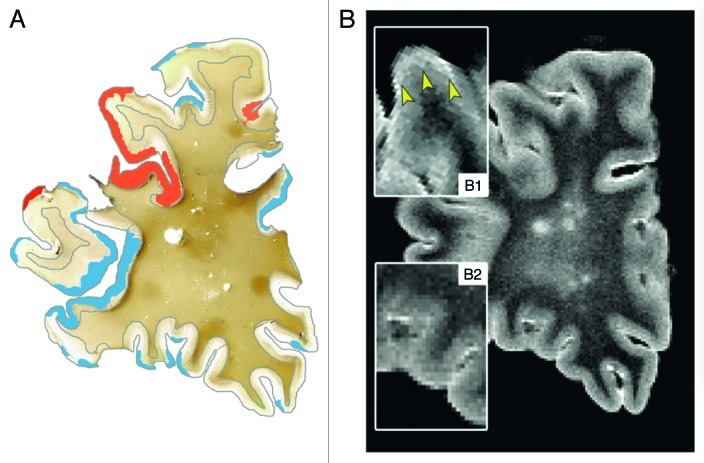
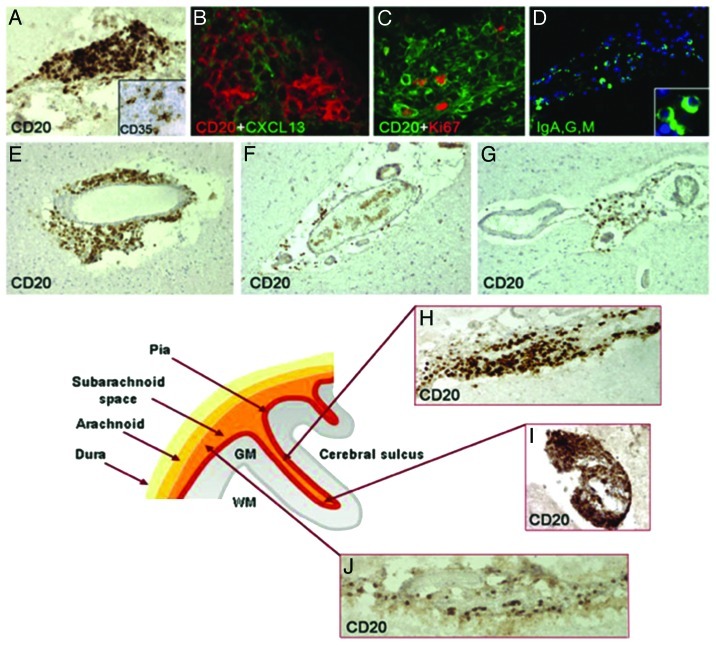
Over the past decade, immunohistochemical studies have provided compelling evidence that gray matter (GM) pathology in multiple sclerosis (MS) is extensive. Until recently, this GM pathology was difficult to visualize using standard magnetic resonance imaging (MRI) techniques. However, with newly developed MRI sequences, it has become clear that GM damage is present from the earliest stages of the disease and accrues with disease progression. GM pathology is clinically relevant, as GM lesions and/or GM atrophy were shown to be associated with MS motor deficits and cognitive impairment. Recent autopsy studies demonstrated significant GM demyelination and microglia activation. However, extensive immune cell influx, complement activation and blood-brain barrier leakage, like in WM pathology, are far less prominent in the GM. Hence, so far, the cause of GM damage in MS remains unknown, although several plausible underlying pathogenic mechanisms have been proposed. This paper provides an overview of GM damage in MS with a focus on its topology and histopathology.
Keywords: clinical relevance; grey matter pathology; imaging; multiple sclerosis; topology.
Figures
References
-
- Cottrell DA, Kremenchutzky M, Rice GP, Koopman WJ, Hader W, Baskerville J, et al. The natural history of multiple sclerosis: a geographically based study. 5. The clinical features and natural history of primary progressive multiple sclerosis. Brain. 1999;122:625–39. doi: 10.1093/brain/122.4.625. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous