

Interspinous spacers compared with decompression or fusion for lumbar stenosis: complications and repeat operations in the Medicare population
- PMID: 23324936
- PMCID: PMC3855445
- DOI: 10.1097/BRS.0b013e31828631b8
Interspinous spacers compared with decompression or fusion for lumbar stenosis: complications and repeat operations in the Medicare population
Abstract
Study design: Retrospective cohort analysis of Medicare claims for 2006-2009.
Objective: To examine whether interspinous distraction procedures are used selectively in patients with more advanced age or comorbidity, and whether they are associated with fewer complications, lower costs, and less revision surgery than laminectomy or fusion surgery.
Summary of background data: A manufacturer-sponsored randomized trial suggested an advantage of interspinous spacer surgery compared with nonsurgical care, but there are few comparisons with other surgical procedures. Furthermore, there are few population-based data evaluating patterns of use of these devices.
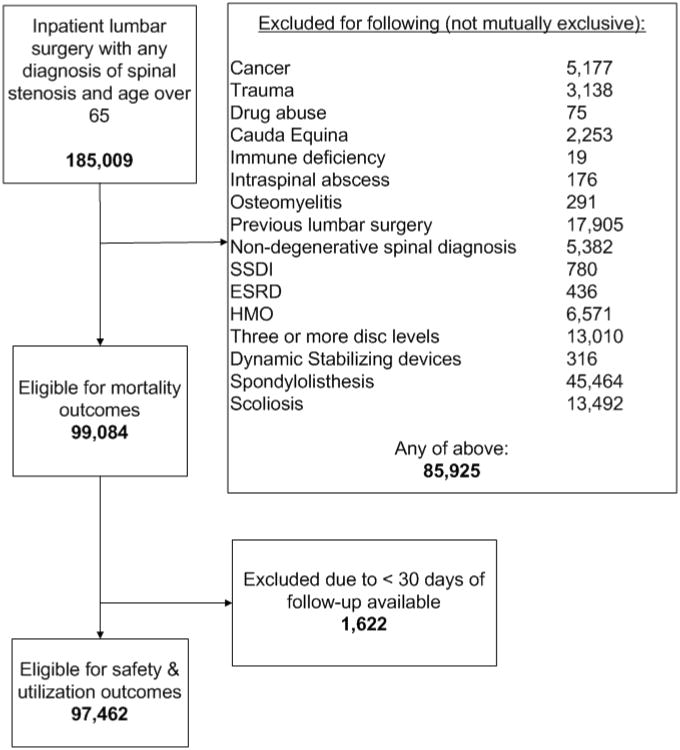
Methods: We used Medicare inpatient claims data to compare age and comorbidity for patients with spinal stenosis undergoing surgery (n = 99,084) with (1) an interspinous process spacer alone; (2) laminectomy and a spacer; (3) decompression alone; or (4) lumbar fusion (1-2 level). We also compared these 4 groups for cost of surgery and rates of revision surgery, major medical complications, wound complications, mortality, and 30-day readmission rates.
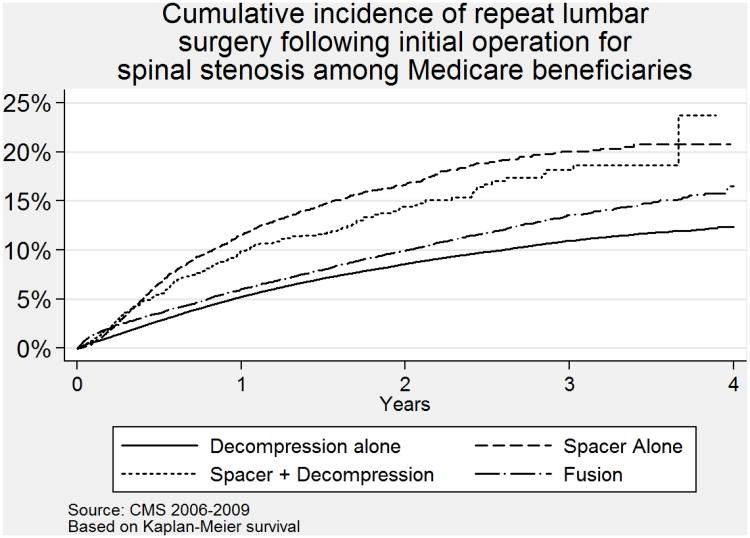
Results: Patients who received spacers were older than those undergoing decompression or fusion, but had little evidence of greater comorbidity. Patients receiving a spacer alone had fewer major medical complications than those undergoing decompression or fusion surgery (1.2% vs. 1.8% and 3.3%, respectively), but had higher rates of further inpatient lumbar surgery (16.7% vs. 8.5% for decompression and 9.8% for fusion at 2 yr). Hospital payments for spacer surgery were greater than those for decompression alone but less than for fusion procedures. These associations persisted in multivariate models adjusting for patient age, sex, comorbidity score, and previous hospitalization.
Conclusion: Compared with decompression or fusion, interspinous distraction procedures pose a trade-off in outcomes: fewer complications for the index operation, but higher rates of revision surgery. This information should help patients make more informed choices, but further research is needed to define optimal indications for these new devices.
Level of evidence: 4.
Figures
References
-
- Zucherman JF, Hsu KY, Hartjen CA, et al. A multicenter, prospective, randomized trial evaluating the X STOP interspinous process decompression system for the treatment of neurogenic intermittent claudication: Two-year follow-up results. Spine. 2005;30:1351–1358. - PubMed
-
- Siddiqui M, Smith FW, Wardlaw D. One year results of X Stop interspinous implant for the treatment of lumbar spinal stenosis. Spine. 2007;32:1345–8. - PubMed
-
- Schermerhorn ML, O'Malley AJ, Jhaveri A, Cotterill P, Pomposelli F, Landon EE. Endovascular vs. open repair of abdominal aortic aneurysms in the Medicare population. N Engl J Med. 2008;358:464–474. - PubMed
-
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360:1418–1428. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
