

Blood urea nitrogen/creatinine ratio identifies a high-risk but potentially reversible form of renal dysfunction in patients with decompensated heart failure
- PMID: 23325460
- PMCID: PMC4067251
- DOI: 10.1161/CIRCHEARTFAILURE.112.968230
Blood urea nitrogen/creatinine ratio identifies a high-risk but potentially reversible form of renal dysfunction in patients with decompensated heart failure
Abstract
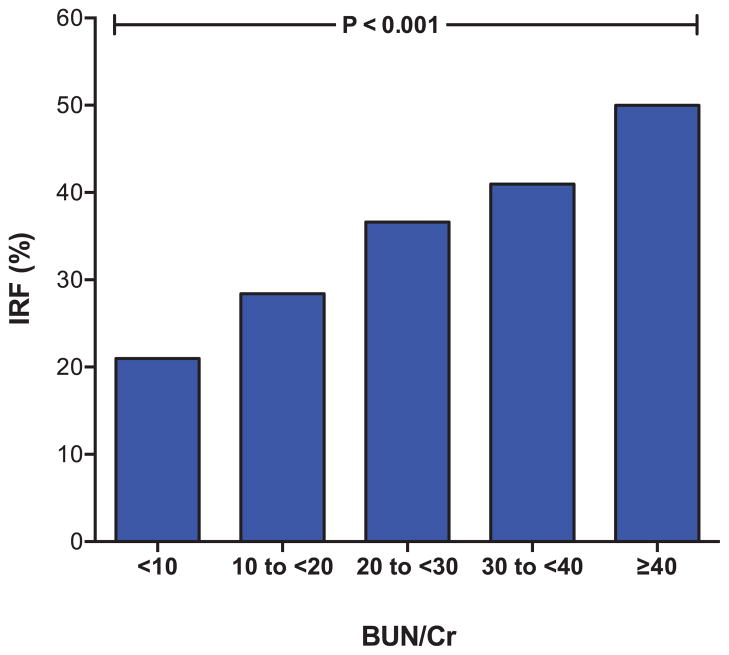
Background: Identifying reversible renal dysfunction (RD) in the setting of heart failure is challenging. The goal of this study was to evaluate whether elevated admission blood urea nitrogen/creatinine ratio (BUN/Cr) could identify decompensated heart failure patients likely to experience improvement in renal function (IRF) with treatment.
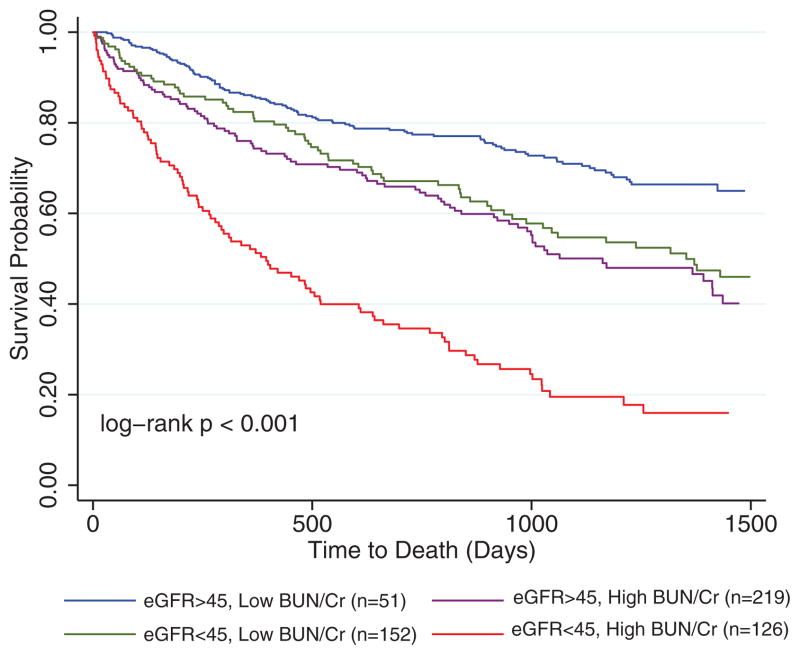
Methods and results: Consecutive hospitalizations with a discharge diagnosis of heart failure were reviewed. IRF was defined as ≥20% increase and worsening renal function as ≥20% decrease in estimated glomerular filtration rate. IRF occurred in 31% of the 896 patients meeting eligibility criteria. Higher admission BUN/Cr was associated with in-hospital IRF (odds ratio, 1.5 per 10 increase; 95% confidence interval [CI], 1.3-1.8; P<0.001), an association persisting after adjustment for baseline characteristics (odds ratio, 1.4; 95% CI, 1.1-1.8; P=0.004). However, higher admission BUN/Cr was also associated with post-discharge worsening renal function (odds ratio, 1.4; 95% CI, 1.1-1.8; P=0.011). Notably, in patients with an elevated admission BUN/Cr, the risk of death associated with RD (estimated glomerular filtration rate <45) was substantial (hazard ratio, 2.2; 95% CI, 1.6-3.1; P<0.001). However, in patients with a normal admission BUN/Cr, RD was not associated with increased mortality (hazard ratio, 1.2; 95% CI, 0.67-2.0; P=0.59; p interaction=0.03).
Conclusions: An elevated admission BUN/Cr identifies decompensated patients with heart failure likely to experience IRF with treatment, providing proof of concept that reversible RD may be a discernible entity. However, this improvement seems to be largely transient, and RD, in the setting of an elevated BUN/Cr, remains strongly associated with death. Further research is warranted to develop strategies for the optimal detection and treatment of these high-risk patients.
Figures
Similar articles
-
Relationship between blood urea nitrogen-to-creatinine ratio at hospital admission and long-term mortality in patients with acute decompensated heart failure.Heart Vessels. 2018 Aug;33(8):877-885. doi: 10.1007/s00380-018-1135-3. Epub 2018 Feb 7. Heart Vessels. 2018. PMID: 29417223
-
A combined-biomarker approach to clinical phenotyping renal dysfunction in heart failure.J Card Fail. 2014 Dec;20(12):912-9. doi: 10.1016/j.cardfail.2014.08.008. Epub 2014 Aug 23. J Card Fail. 2014. PMID: 25152498 Free PMC article.
-
Ratio of blood urea nitrogen to serum creatinine at initiation of dialysis is associated with mortality: a multicenter prospective cohort study.Clin Exp Nephrol. 2018 Apr;22(2):353-364. doi: 10.1007/s10157-017-1458-x. Epub 2017 Aug 1. Clin Exp Nephrol. 2018. PMID: 28766029
-
Renal dysfunction in acute heart failure: epidemiology, mechanisms and assessment.Heart Fail Rev. 2012 Mar;17(2):271-82. doi: 10.1007/s10741-011-9265-z. Heart Fail Rev. 2012. PMID: 21748453 Review.
-
Epidemiology and importance of renal dysfunction in heart failure patients.Curr Heart Fail Rep. 2013 Dec;10(4):411-20. doi: 10.1007/s11897-013-0164-6. Curr Heart Fail Rep. 2013. PMID: 24097112 Review.
Cited by
-
The prognostic role of urea-to-creatinine ratio in patients with acute heart failure syndrome: a case-control study.Egypt Heart J. 2023 Sep 5;75(1):78. doi: 10.1186/s43044-023-00404-y. Egypt Heart J. 2023. PMID: 37668813 Free PMC article.
-
Blood urea nitrogen/creatinine ratio in heart failure: Systematic review and meta-analysis.PLoS One. 2024 May 28;19(5):e0303870. doi: 10.1371/journal.pone.0303870. eCollection 2024. PLoS One. 2024. PMID: 38805436 Free PMC article.
-
Relevance of Changes in Serum Creatinine During a Heart Failure Trial of Decongestive Strategies: Insights From the DOSE Trial.J Card Fail. 2016 Oct;22(10):753-60. doi: 10.1016/j.cardfail.2016.06.423. Epub 2016 Jun 30. J Card Fail. 2016. PMID: 27374839 Free PMC article. Clinical Trial.
-
Elevated serum urea-to-creatinine ratio is associated with adverse inpatient clinical outcomes in non-end stage chronic kidney disease.Sci Rep. 2022 Dec 2;12(1):20827. doi: 10.1038/s41598-022-25254-7. Sci Rep. 2022. PMID: 36460694 Free PMC article.
-
Association of blood urea nitrogen to creatinine ratio with incident type 2 diabetes mellitus: A retrospective cohort study in the Chinese population.Medicine (Baltimore). 2024 Jul 26;103(30):e39003. doi: 10.1097/MD.0000000000039003. Medicine (Baltimore). 2024. PMID: 39058804 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
