

Renal cell carcinoma metastases to the pancreas: value of arterial phase imaging at MDCT
- PMID: 23325783
- PMCID: PMC10919206
- DOI: 10.1258/ar.2012.120693
Renal cell carcinoma metastases to the pancreas: value of arterial phase imaging at MDCT
Abstract
Background: The pancreas is an increasingly recognized site of renal cell carcinoma metastases. It is important to determine the optimal MDCT protocol to best detect RCC metastases to the pancreas.
Purpose: To compare the rate of detection of renal cell carcinoma metastases to the pancreas between arterial and portal venous phase MDCT.
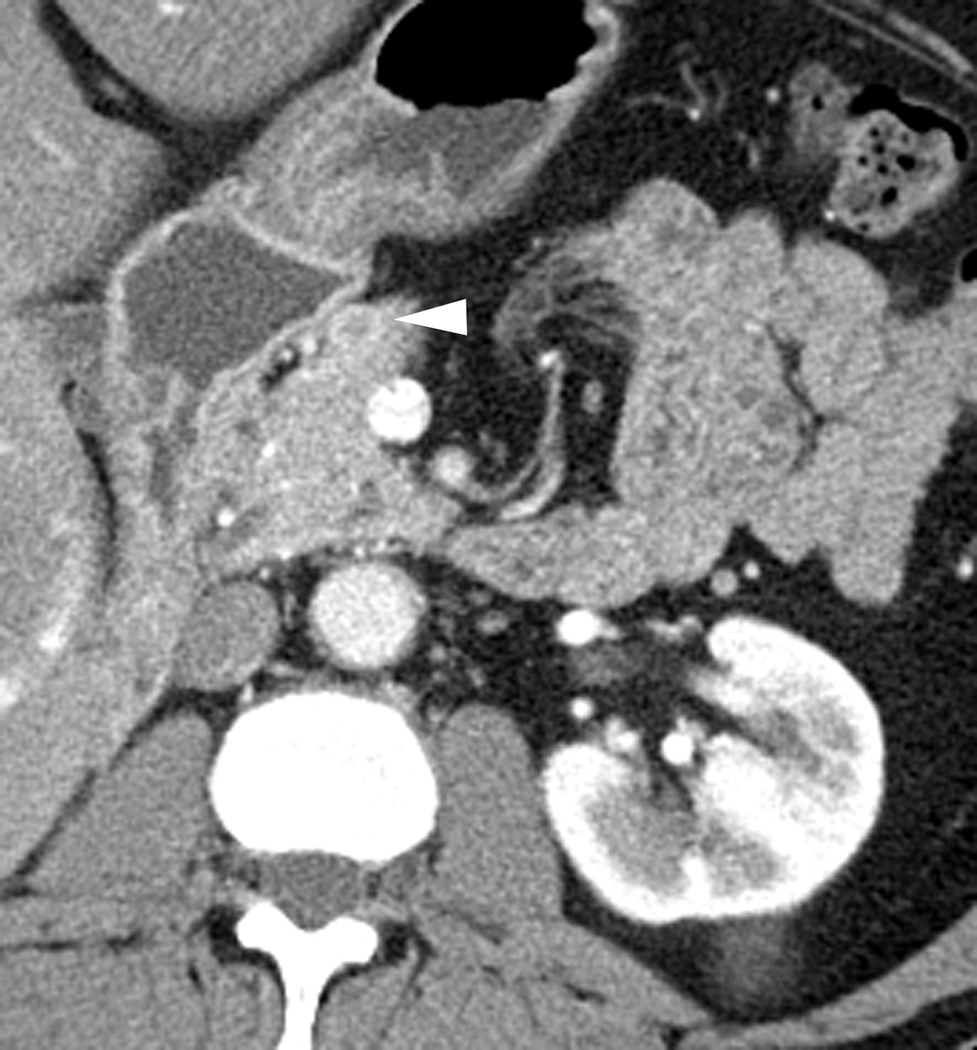
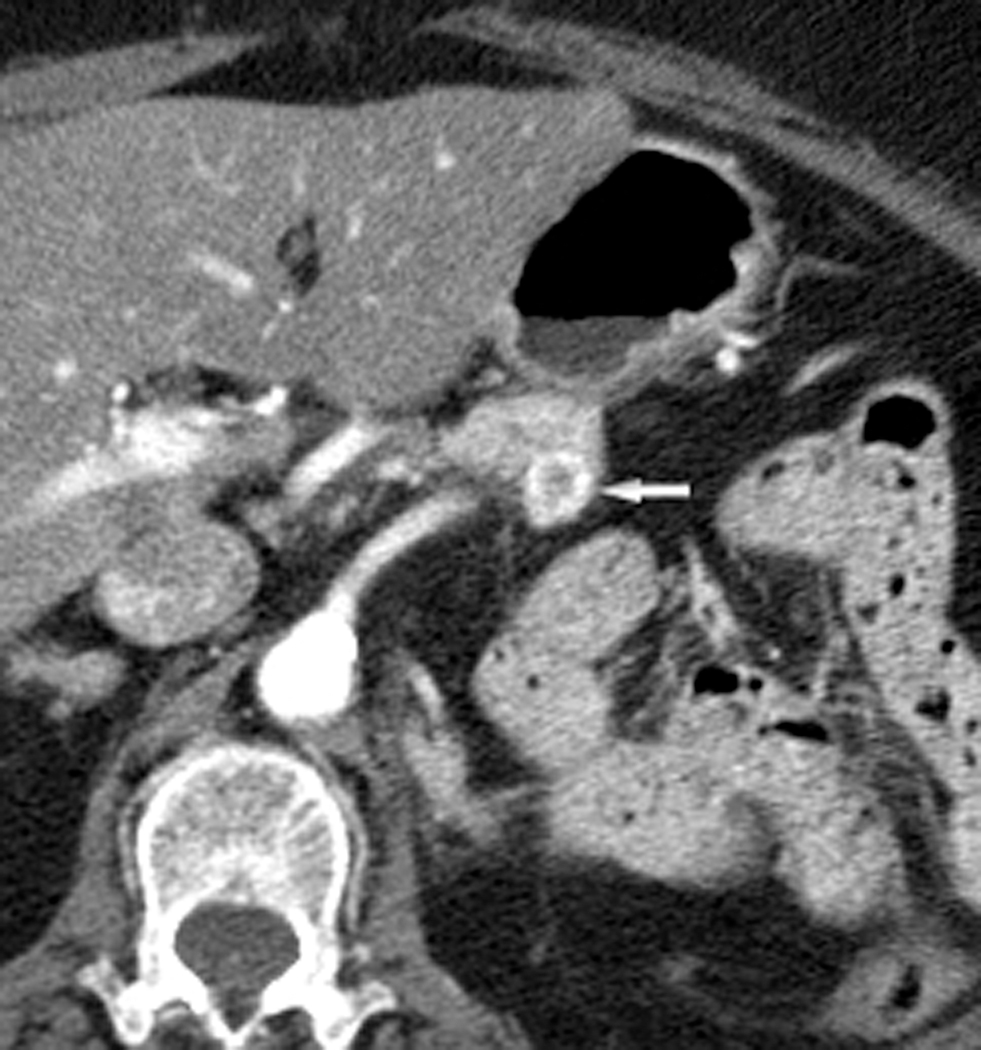
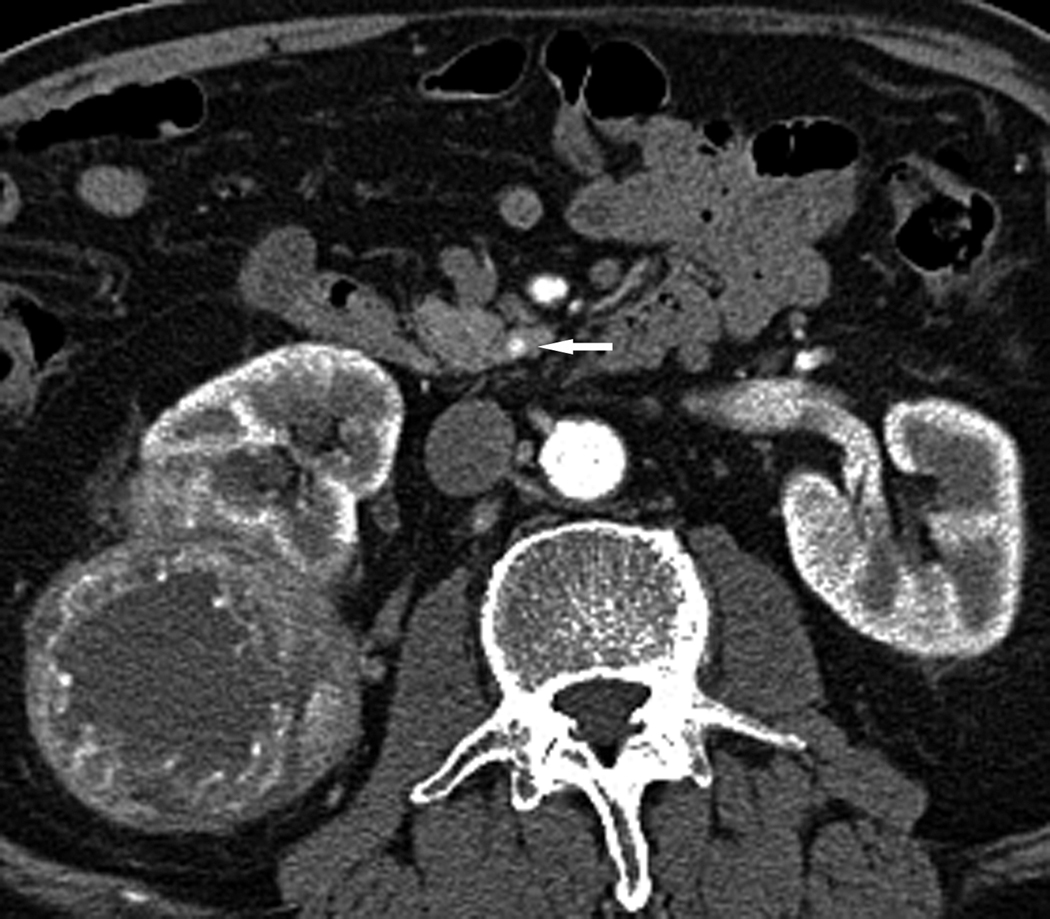
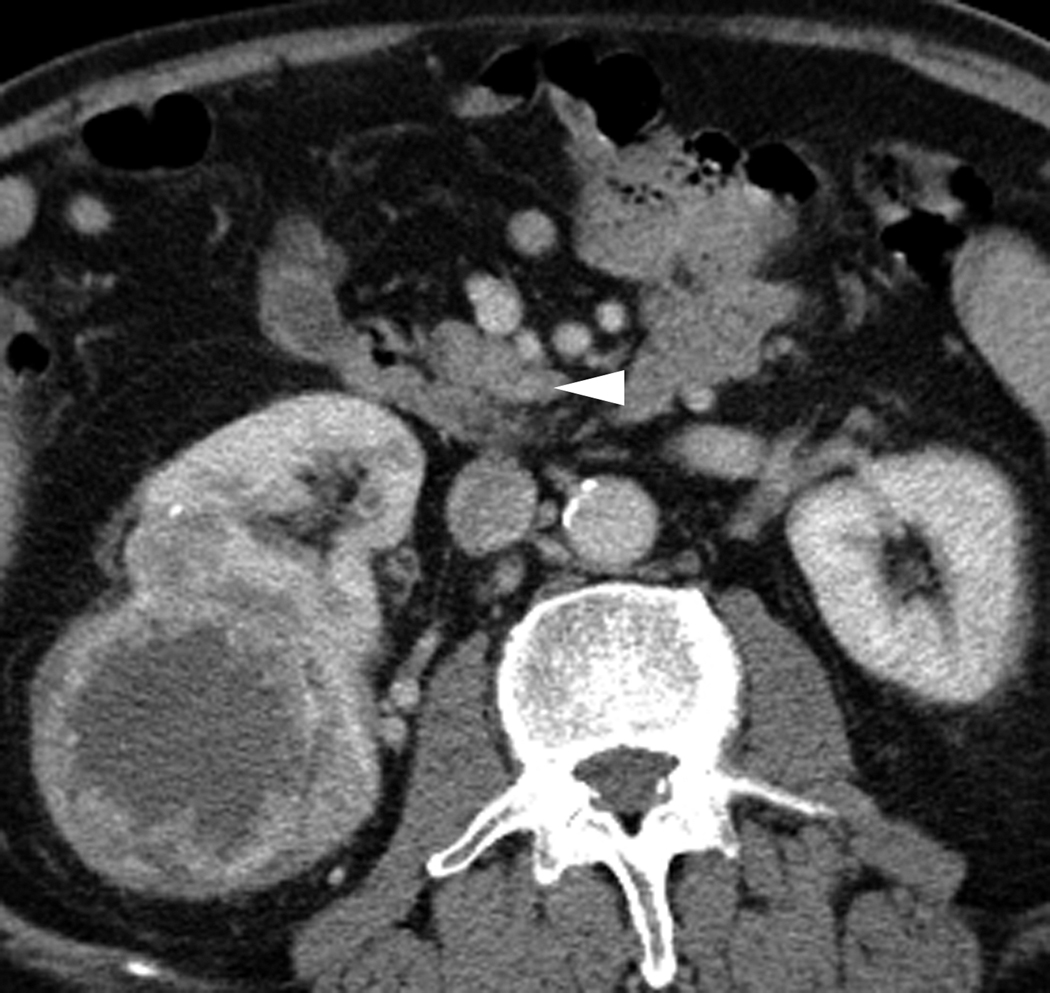
Material and methods: A retrospective review of CTs of the abdomen yielded six patients with metastatic RCC to the pancreas. Five of six patients had pathologically proven clear cell RCC. Two blinded reviewers independently reported the number of pancreatic lesions seen in arterial and venous phases. Each lesion was graded as definite or possible. The number of lesions was determined by consensus review of both phases. Attenuation values were obtained for metastatic lesions and adjacent normal pancreas in both phases.
Results: There were a total of 24 metastatic lesions to the pancreas. Reviewer 1 identified 20/24 (83.3%) lesions on the arterial phase images and 13/24 (54.2%) lesions on the venous phase. Seventeen of 20 (85.0%) arterial lesions were deemed definite and 9/13 (69.2%) venous lesions were definite. Reviewer 2 identified 19/24 (79.2%) lesions on the arterial phase and 14/24 (58.3%) on the venous phase. Seventeen of 19 (89.5%) arterial lesions were definite and 7/14 (50%) venous lesions were definite. Mean attenuation differential between lesion and pancreas was 114 HU and 39 HU for arterial and venous phases, respectively (P<0.0001).
Conclusion: Detection of RCC metastases to the pancreas at MDCT is improved using arterial phase imaging compared to portal venous phase imaging.
Figures


Similar articles
-
Metastases to the pancreas from renal cell carcinoma: findings on three-phase contrast-enhanced helical CT.AJR Am J Roentgenol. 1999 Jun;172(6):1555-9. doi: 10.2214/ajr.172.6.10350288. AJR Am J Roentgenol. 1999. PMID: 10350288
-
Is dual-phase abdominal CT necessary for the optimal detection of metastases from renal cell carcinoma?Clin Radiol. 2011 Nov;66(11):1055-9. doi: 10.1016/j.crad.2011.06.002. Epub 2011 Aug 16. Clin Radiol. 2011. PMID: 21843882
-
Renal cell carcinoma metastatic to the pancreas: clinical and radiological features.Mayo Clin Proc. 2000 Jun;75(6):581-5. doi: 10.4065/75.6.581. Mayo Clin Proc. 2000. PMID: 10852418
-
Metastatic renal cell carcinoma to pancreas and gastrointestinal tract: a clinicopathological study of 3 cases and review of literature.BMC Urol. 2021 May 25;21(1):84. doi: 10.1186/s12894-021-00854-z. BMC Urol. 2021. PMID: 34034720 Free PMC article. Review.
-
Renal cell carcinoma to the pancreas in surgical pathology material.Cancer. 2000 Sep 1;89(5):1076-88. doi: 10.1002/1097-0142(20000901)89:5<1076::aid-cncr17>3.0.co;2-m. Cancer. 2000. PMID: 10964338 Review.
Cited by
-
Is a single portal venous phase in contrast-enhanced CT sufficient to detect metastases or recurrence in clear cell renal cell carcinoma? - a single-center retrospective study.Cancer Imaging. 2022 Jan 21;22(1):9. doi: 10.1186/s40644-022-00444-8. Cancer Imaging. 2022. PMID: 35063030 Free PMC article.
-
Metastases to the Pancreas: Computed Tomography Imaging Spectrum and Clinical Features: A Retrospective Study of 18 Patients With 36 Metastases.Medicine (Baltimore). 2015 Jun;94(23):e913. doi: 10.1097/MD.0000000000000913. Medicine (Baltimore). 2015. PMID: 26061312 Free PMC article.
-
Development of CT-Based Imaging Signature for Preoperative Prediction of Invasive Behavior in Pancreatic Solid Pseudopapillary Neoplasm.Front Oncol. 2021 May 17;11:677814. doi: 10.3389/fonc.2021.677814. eCollection 2021. Front Oncol. 2021. PMID: 34079766 Free PMC article.
-
(18)F-FDG-PET/CT findings in pancreatic metastasis.Radiol Med. 2015 Oct;120(10):887-98. doi: 10.1007/s11547-014-0473-1. Epub 2015 Mar 22. Radiol Med. 2015. PMID: 25795439
References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin 2012; 62:10–29 - PubMed
-
- Patel U, Sokhi H. Imaging in the follow-up of renal cell carcinoma. Am J Roentgenol 2012; 198:1266–76 - PubMed
-
- Tanis PJ, van der Gaag NA, Busch OR, et al. Systematic review of pancreatic surgery for metastatic renal cell carcinoma. BrJ Surg 2009; 96:579–92 - PubMed
-
- Mecho S, Quiroga S, Cuellar H, et al. Pancreatic metastasis of renal cell carcinoma: multidetector CT findings. Abdom Imaging 2009; 34:385–9 - PubMed
-
- Robbins EG, 2nd, Franceschi D, Barkin JS. Solitary metastatic tumors to the pancreas: a case report and review of the literature. Am J Gastroenterol 1996; 91:2414–7 - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
