A review of the practice of sedation with inhalational anaesthetics in the intensive care unit with the AnaConDa(®) device
- PMID: 23325934
- PMCID: PMC3546236
- DOI: 10.4103/0019-5049.104565
A review of the practice of sedation with inhalational anaesthetics in the intensive care unit with the AnaConDa(®) device
Abstract
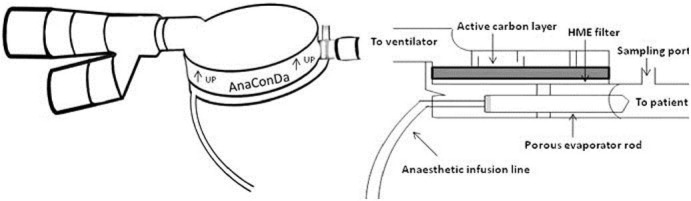
The intensive care unit (ICU) environment is often perceived to be hostile and frightening by patients due to unfamiliar surroundings coupled with presence of numerous personnel, monitors and other equipments as well as a loss of perception of time. Mechanical ventilation and multiple painful procedures that often need to be carried out in these critically ill patients add to their overall anxiety. Sedation is therefore required not only to allay the stress and anxiety, but also to allow for mechanical ventilation and other invasive therapeutic and diagnostic procedures to be performed. The conventional intravenous sedative agents used in ICUs suffer from problems of over sedation, tachyphylaxis, drug accumulation, organ specific elimination and often lead to patient agitation on withdrawal. All this tend to prolong the ventilatory as well as ICU and hospital discharge time, which increase the risk for infection and add to the overall increase in morbidity, mortality and hospital costs. In 2005, the anaesthetic conserving device (AnaConDa(®)) was marketed for ICU sedation with volatile anaesthetic agents. A number of trials have shown the effectiveness of using volatile anaesthetic agents for ICU sedation with the AnaConDa device. Compared with intravenous sedatives, use of volatile anaesthetic agents have resulted in shorter wake up and extubation time, lesser duration of mechanical ventilation and faster discharge from hospitals. This review shall focus on the benefits, technical pre-requisites and status of sedation with volatile anaesthetic agents in ICUs with the AnaConDa(®) device.
Keywords: Anaesthetic conserving device; ICU sedation; isoflurane; midazolam; propofol; sevoflurane.
Conflict of interest statement
Figures
Similar articles
-
The advantages of inhalational sedation using an anesthetic-conserving device versus intravenous sedatives in an intensive care unit setting: A systematic review.Ann Thorac Med. 2023 Oct-Dec;18(4):182-189. doi: 10.4103/atm.atm_89_23. Epub 2023 Oct 17. Ann Thorac Med. 2023. PMID: 38058786 Free PMC article. Review.
-
Inhalational anaesthetics in the ICU: theory and practice of inhalational sedation in the ICU, economics, risk-benefit.Best Pract Res Clin Anaesthesiol. 2005 Sep;19(3):523-38. doi: 10.1016/j.bpa.2005.02.006. Best Pract Res Clin Anaesthesiol. 2005. PMID: 16013698 Review.
-
A technical review of the history, development and performance of the anaesthetic conserving device "AnaConDa" for delivering volatile anaesthetic in intensive and post-operative critical care.J Clin Monit Comput. 2018 Aug;32(4):595-604. doi: 10.1007/s10877-017-0097-9. Epub 2018 Jan 31. J Clin Monit Comput. 2018. PMID: 29388094 Free PMC article. Review.
-
Safety and effectiveness of inhaled sedation in critically ill patients: a systematic review and meta-analysis.Syst Rev. 2025 Feb 19;14(1):44. doi: 10.1186/s13643-025-02791-6. Syst Rev. 2025. PMID: 39972505 Free PMC article.
-
[Functioning of the anaesthetic conserving device: aspects to consider for use in inhalational sedation].Anaesthesist. 2010 Nov;59(11):1029-40. doi: 10.1007/s00101-010-1779-6. Anaesthesist. 2010. PMID: 20878139 German.
Cited by
-
Efficient application of volatile anaesthetics: total rebreathing or specific reflection?J Clin Monit Comput. 2018 Aug;32(4):615-622. doi: 10.1007/s10877-017-0096-x. Epub 2018 Jan 4. J Clin Monit Comput. 2018. PMID: 29302897 Review.
-
A novel device for target controlled administration and reflection of desflurane--the Mirus™.Anaesthesia. 2014 Nov;69(11):1241-50. doi: 10.1111/anae.12798. Epub 2014 Jul 9. Anaesthesia. 2014. PMID: 25040673 Free PMC article.
-
Volatile anaesthetic for treatment of respiratory failure from status asthmaticus requiring extracorporeal membrane oxygenation.BMJ Case Rep. 2020 Jan 15;13(1):e231507. doi: 10.1136/bcr-2019-231507. BMJ Case Rep. 2020. PMID: 31948977 Free PMC article.
-
Seizures - just the tip of the iceberg: Critical care management of super-refractory status epilepticus.Indian J Crit Care Med. 2016 Oct;20(10):587-592. doi: 10.4103/0972-5229.192047. Indian J Crit Care Med. 2016. PMID: 27829714 Free PMC article. Review.
-
The advantages of inhalational sedation using an anesthetic-conserving device versus intravenous sedatives in an intensive care unit setting: A systematic review.Ann Thorac Med. 2023 Oct-Dec;18(4):182-189. doi: 10.4103/atm.atm_89_23. Epub 2023 Oct 17. Ann Thorac Med. 2023. PMID: 38058786 Free PMC article. Review.
References
-
- Shapiro BA, Warren J, Egol AB, Greenbaum DM, Jacobi J, Nasraway SA, et al. Practice parameters for intravenous analgesia and sedation for adult patients in the intensive care unit: An executive summary. Society of Critical Care Medicine. Crit Care Med. 1995;23:1596–600. - PubMed
-
- Jacobi J, Fraser GL, Coursin DB, Riker RR, Fontaine D, Wittbrodt ET, et al. Task Force of the American College of Critical Care Medicine (ACCM) of the Society of Critical Care Medicine (SCCM), American Society of Health-System Pharmacists (ASHP), American College of Chest Physicians.Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adult. Crit Care Med. 2002;30:119–41. - PubMed
-
- Vasile B, Rasulo F, Candiani A, Latronico N. The pathophysiology of propofol infusion syndrome: A simple name for a complex syndrome. Intensive Care Med. 2003;29:1417–25. - PubMed
-
- Shafer A. Complications of sedation with midazolam in the intensive care unit and a comparison with other sedative regimens. Crit Care Med. 1998;26:947–56. - PubMed
-
- Wagner RL, White PF. Etomidate inhibits adrenocortical function in surgical patients. Anesthesiology. 1984;61:647–51. - PubMed