

Alcohol, postprandial plasma glucose, and prognosis of hepatocellular carcinoma
- PMID: 23326166
- PMCID: PMC3542757
- DOI: 10.3748/wjg.v19.i1.78
Alcohol, postprandial plasma glucose, and prognosis of hepatocellular carcinoma
Abstract
Aim: To identify factors associated with prognosis of hepatocellular carcinoma (HCC) after initial therapy.
Methods: A total of 377 HCC patients who were newly treated at Katsushika Medical Center, Japan from January 2000 to December 2009 and followed up for > 2 years, or died during follow-up, were enrolled. The factors related to survival were first analyzed in 377 patients with HCC tumor stage T1-T4 using multivariate Cox proportional hazards regression analysis. A similar analysis was performed in 282 patients with tumor stage T1-T3. Additionally, factors associated with the period between initial and subsequent therapy were examined in 144 patients who did not show local recurrence. Finally, 214 HCC stage T1-T3 patients who died during the observation period were classified into four groups according to their alcohol consumption and postprandial glucose levels, and differences in their causes of death were examined.
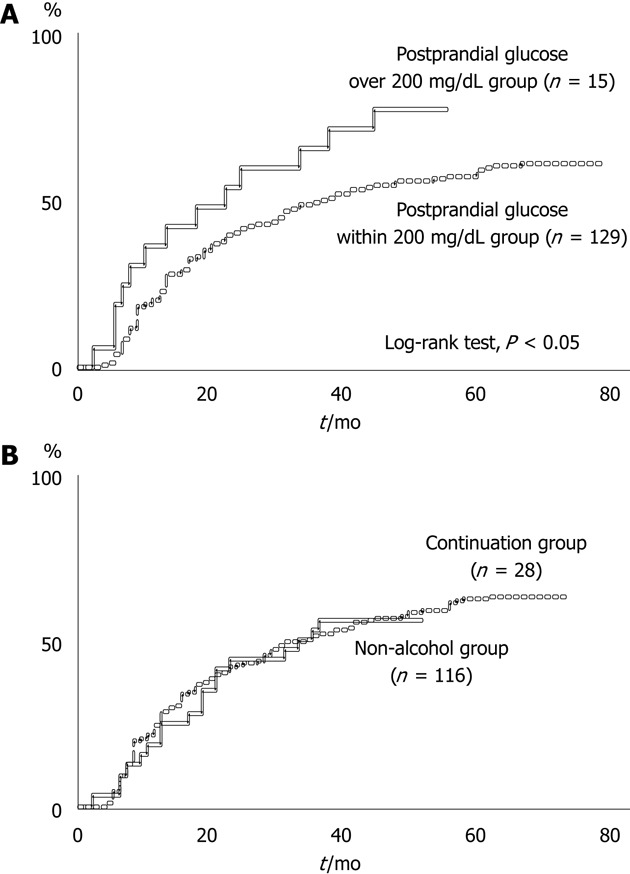
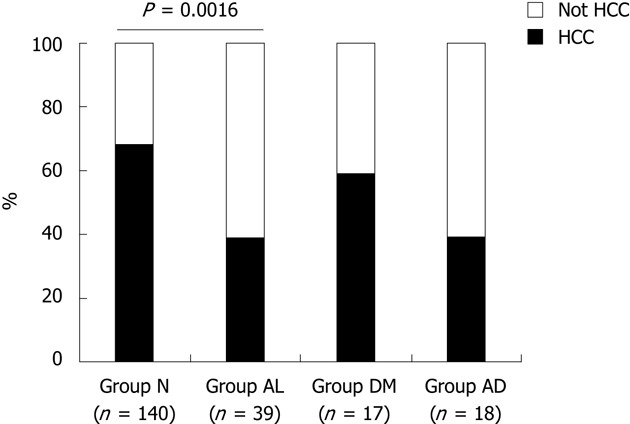
Results: On multivariate Cox proportional hazards regression analysis, the following were significantly associated with survival: underlying liver disease stage [non-cirrhosis/Child-Pugh A vs B/C, hazard ratio (HR): 0.603, 95% CI: 0.417-0.874, P = 0.0079], HCC stage (T1/T2 vs T3/T4, HR: 0.447, 95% CI: 0.347-0.576, P < 0.0001), and mean postprandial plasma glucose after initial therapy (< 200 vs ≥ 200 mg/dL, HR: 0.181, 95% CI: 0.067-0.488, P = 0.0008). In T1-T3 patients, uninterrupted alcohol consumption after initial therapy (no vs yes, HR: 0.641, 95% CI: 0.469-0.877, P = 0.0055) was significant in addition to underlying liver disease stage (non-cirrhosis/Child-Pugh A vs B/C, HR: 0649, 95% CI: 0.476-0.885, P = 0.0068), HCC stage (T1 vs T2/T3, HR: 0.788, 95% CI: 0.653-0.945, P = 0.0108), and mean postprandial plasma glucose after initial therapy (< 200 mg/dL vs ≥ 200 mg/dL, HR: 0.502, 95% CI: 0.337-0.747, P = 0.0005). In patients without local recurrence, time from initial to subsequent therapy for newly emerging HCC was significantly longer in the "postprandial glucose within 200 mg/dL group" than the "postprandial glucose > 200 mg/dL group" (log-rank test, P < 0.05), whereas there was no difference in the period between the "non-alcohol group" (patients who did not drink regularly or those who could reduce their daily consumption to < 20 g) and the "continuation group" (drinkers who continued to drink > 20 g daily). Of 214 T1-T3 patients who died during the observation period, death caused by other than HCC progression was significantly more frequent in "group AL" (patients in the continuation and postprandial glucose within 200 mg/dL groups) than "group N" (patients in the non-alcohol and postprandial glucose within 200 mg/dL groups) (P = 0.0016).
Conclusion: This study found that abstinence from habitual alcohol consumption and intensive care for diabetes mellitus were related to improved prognosis in HCC patients.
Keywords: Alcohol consumption; Diabetes mellitus; Hepatocellular carcinoma; Initial therapy; Local recurrence; Postprandial plasma glucose level; Prognosis; Survival.
Figures
References
-
- Seeff LB, Hoofnagle JH. Epidemiology of hepatocellular carcinoma in areas of low hepatitis B and hepatitis C endemicity. Oncogene. 2006;25:3771–3777. - PubMed
-
- Ikeda K, Saitoh S, Koida I, Arase Y, Tsubota A, Chayama K, Kumada H, Kawanishi M. A multivariate analysis of risk factors for hepatocellular carcinogenesis: a prospective observation of 795 patients with viral and alcoholic cirrhosis. Hepatology. 1993;18:47–53. - PubMed
-
- Bruix J, Sherman M, Llovet JM, Beaugrand M, Lencioni R, Burroughs AK, Christensen E, Pagliaro L, Colombo M, Rodés J. Clinical management of hepatocellular carcinoma. Conclusions of the Barcelona-2000 EASL conference. European Association for the Study of the Liver. J Hepatol. 2001;35:421–430. - PubMed
-
- Ikai I, Itai Y, Okita K, Omata M, Kojiro M, Kobayashi K, Nakanuma Y, Futagawa S, Makuuchi M, Yamaoka Y. Report of the 15th follow-up survey of primary liver cancer. Hepatol Res. 2004;28:21–29. - PubMed
-
- Noguchi K, Nakashima O, Nakashima Y, Shiota K, Nawata H, Kojiro M. Clinicopathologic study on hepatocellular carcinoma negative for hepatitis B surface antigen and antibody to hepatitis C virus. Int J Mol Med. 2000;6:661–665. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
