

Diagnosis and management of miliary tuberculosis: current state and future perspectives
- PMID: 23326198
- PMCID: PMC3544391
- DOI: 10.2147/TCRM.S29179
Diagnosis and management of miliary tuberculosis: current state and future perspectives
Retraction in
-
Diagnosis and management of miliary tuberculosis: current state and future perspectives [Retraction].Ther Clin Risk Manag. 2015 Sep 28;11:1457. doi: 10.2147/TCRM.S96338. eCollection 2015. Ther Clin Risk Manag. 2015. PMID: 26445545 Free PMC article.
Abstract
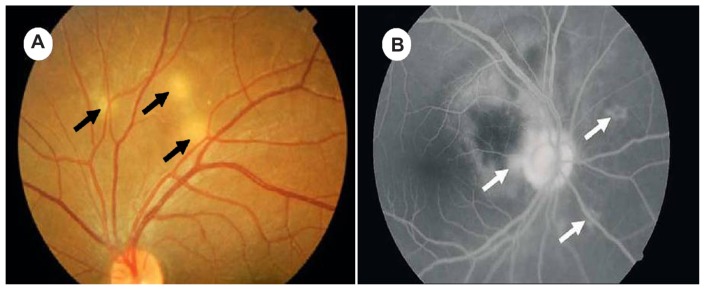
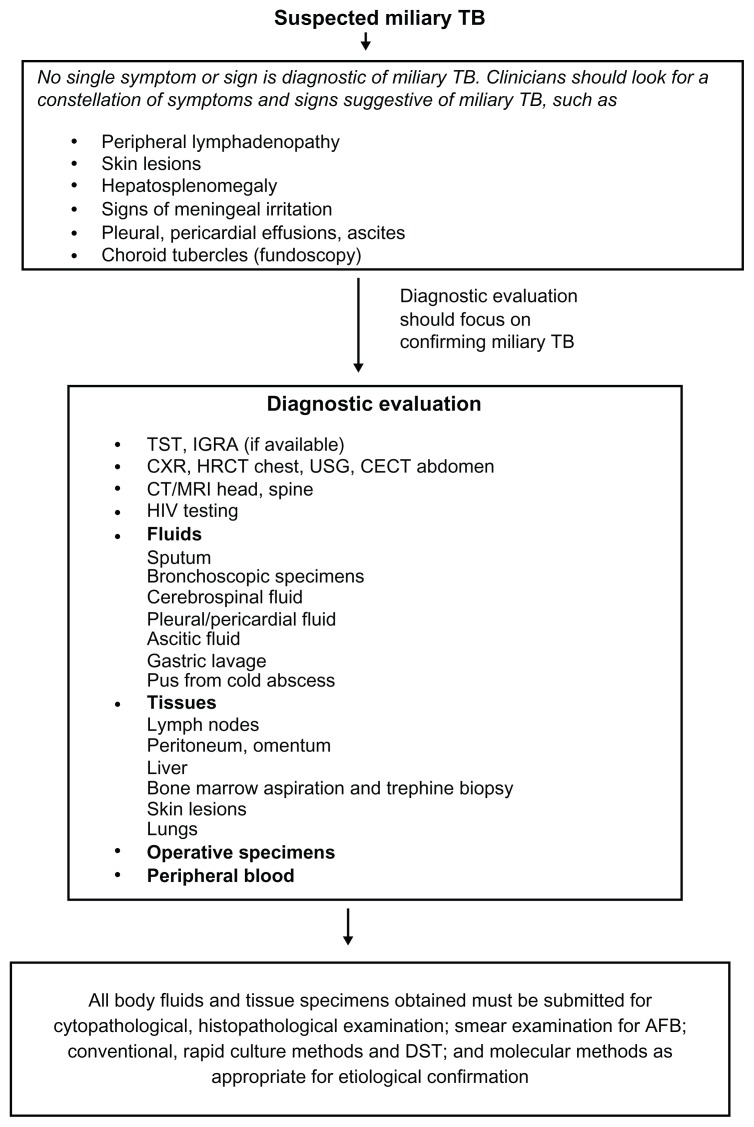
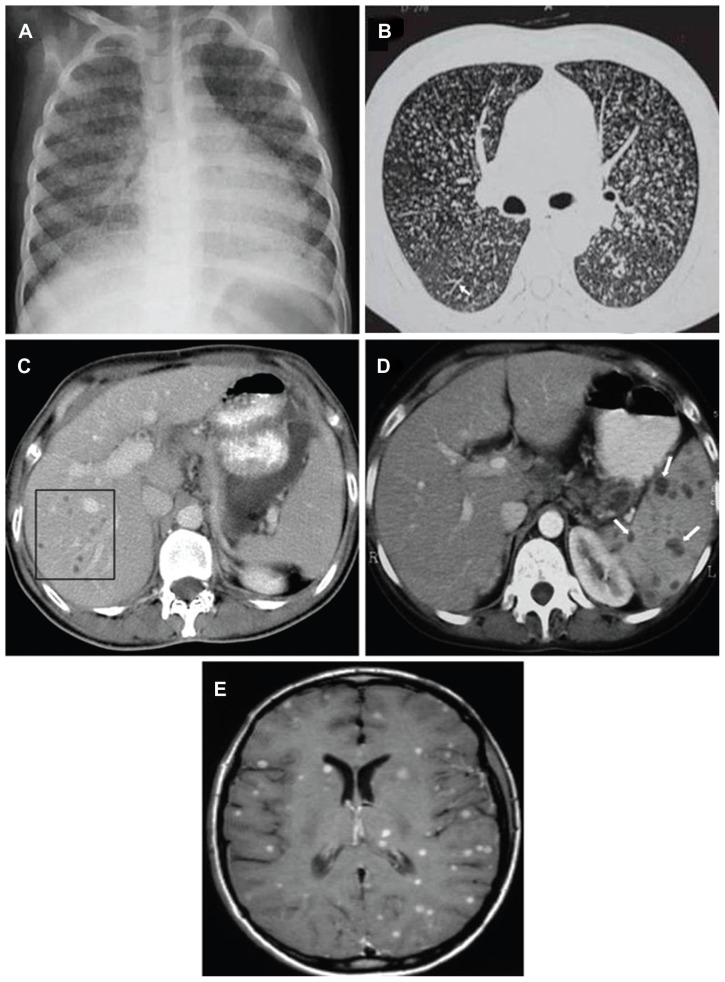
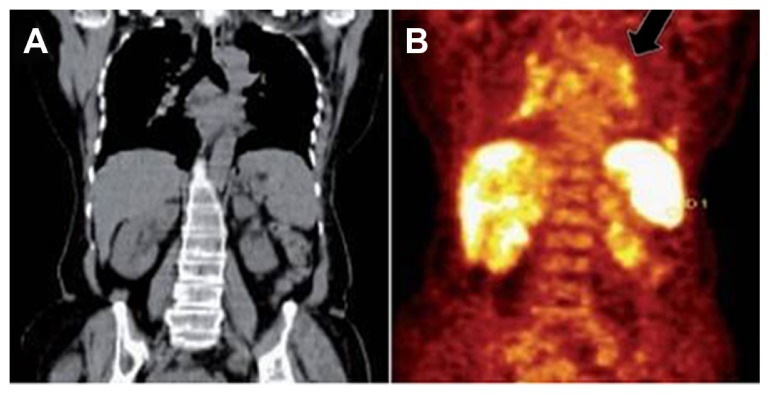
Tuberculosis (TB) remains one of the most important causes of death from an infectious disease, and it poses formidable challenges to global health at the public health, scientific, and political level. Miliary TB is a potentially fatal form of TB that results from massive lymphohematogenous dissemination of Mycobacterium tuberculosis bacilli. The epidemiology of miliary TB has been altered by the emergence of the human immunodeficiency virus (HIV) infection and widespread use of immunosuppressive drugs. Diagnosis of miliary TB is a challenge that can perplex even the most experienced clinicians. There are nonspecific clinical symptoms, and the chest radiographs do not always reveal classical miliary changes. Atypical presentations like cryptic miliary TB and acute respiratory distress syndrome often lead to delayed diagnosis. High-resolution computed tomography (HRCT) is relatively more sensitive and shows randomly distributed miliary nodules. In extrapulmonary locations, ultrasonography, CT, and magnetic resonance imaging are useful in discerning the extent of organ involvement by lesions of miliary TB. Recently, positron-emission tomographic CT has been investigated as a promising tool for evaluation of suspected TB. Fundus examination for choroid tubercles, histopathological examination of tissue biopsy specimens, and rapid culture methods for isolation of M. tuberculosis in sputum, body fluids, and other body tissues aid in confirming the diagnosis. Several novel diagnostic tests have recently become available for detecting active TB disease, screening for latent M. tuberculosis infection, and identifying drug-resistant strains of M. tuberculosis. However, progress toward a robust point-of-care test has been limited, and novel biomarker discovery remains challenging. A high index of clinical suspicion and early diagnosis and timely institution of antituberculosis treatment can be lifesaving. Response to first-line antituberculosis drugs is good, but drug-induced hepatotoxicity and drug-drug interactions in HIV/TB coinfected patients create significant problems during treatment. Data available from randomized controlled trials are insufficient to define the optimum regimen and duration of treatment in patients with drug-sensitive as well as drug-resistant miliary TB, including those with HIV/AIDS, and the role of adjunctive corticosteroid treatment has not been properly studied. Research is going on worldwide in an attempt to provide a more effective vaccine than bacille Calmette-Guérin. This review highlights the epidemiology and clinical manifestation of miliary TB, challenges, recent advances, needs, and opportunities related to TB diagnostics and treatment.
Keywords: Mycobacterium tuberculosis; antituberculosis drugs; biomarkers; diagnostic tests; human immunodeficiency virus; vaccine.
Figures
Similar articles
-
Challenges in the diagnosis & treatment of miliary tuberculosis.Indian J Med Res. 2012 May;135(5):703-30. Indian J Med Res. 2012. PMID: 22771605 Free PMC article. Review.
-
Miliary Tuberculosis.Microbiol Spectr. 2017 Mar;5(2):10.1128/microbiolspec.tnmi7-0013-2016. doi: 10.1128/microbiolspec.TNMI7-0013-2016. Microbiol Spectr. 2017. PMID: 28281441 Free PMC article. Review.
-
Miliary tuberculosis: A new look at an old foe.J Clin Tuberc Other Mycobact Dis. 2016 Mar 18;3:13-27. doi: 10.1016/j.jctube.2016.03.003. eCollection 2016 May. J Clin Tuberc Other Mycobact Dis. 2016. PMID: 31723681 Free PMC article. Review.
-
Miliary tuberculosis: new insights into an old disease.Lancet Infect Dis. 2005 Jul;5(7):415-30. doi: 10.1016/S1473-3099(05)70163-8. Lancet Infect Dis. 2005. PMID: 15978528 Review.
-
API TB Consensus Guidelines 2006: Management of pulmonary tuberculosis, extra-pulmonary tuberculosis and tuberculosis in special situations.J Assoc Physicians India. 2006 Mar;54:219-34. J Assoc Physicians India. 2006. PMID: 16800350
Cited by
-
[Clinical effects of partially de-epithelized local flaps in repairing tubercular chest wall defects].Zhonghua Shao Shang Za Zhi. 2021 Dec 20;37(12):1110-1115. doi: 10.3760/cma.j.cn501120-20210929-00337. Zhonghua Shao Shang Za Zhi. 2021. PMID: 34937152 Free PMC article. Chinese.
-
Miliary Nodules in the Lungs Not Always Due to Tuberculosis: A Report of a Rare Case.Cureus. 2025 Mar 5;17(3):e80120. doi: 10.7759/cureus.80120. eCollection 2025 Mar. Cureus. 2025. PMID: 40190950 Free PMC article.
-
When the Lightning Strikes Twice: Navigating the Complex Terrain of Cerebral Tuberculosis.Cureus. 2024 Jan 11;16(1):e52090. doi: 10.7759/cureus.52090. eCollection 2024 Jan. Cureus. 2024. PMID: 38344590 Free PMC article.
-
Unveiling the Silent Invader: A Case Report on Miliary Tuberculosis.Cureus. 2023 Jul 13;15(7):e41817. doi: 10.7759/cureus.41817. eCollection 2023 Jul. Cureus. 2023. PMID: 37575864 Free PMC article.
-
An unusual presentation of miliary tuberculosis.BMJ Case Rep. 2014 Apr 19;2014:bcr2013202947. doi: 10.1136/bcr-2013-202947. BMJ Case Rep. 2014. PMID: 24748138 Free PMC article.
References
-
- World Health Organization. WHO Report: Global Tuberculosis Control. Geneva: World Health Organization; 2011.
-
- Murray CJ, Lopez AD. Global mortality, disability, and the contribution of risk factors: Global Burden of Disease Study. Lancet. 1997;349:1436–1442. - PubMed
-
- Sahn SA, Neff TA. Miliary tuberculosis. Am J Med. 1974;56:495–505. - PubMed
-
- Sharma SK, Mohan A. Disseminated and miliary tuberculosis. In: Sharma SK, Mohan A, editors. Tuberculosis. 2nd ed. New Delhi: Jaypee Brothers; 2009. pp. 493–518.
-
- Baker SK, Glassroth J. Miliary tuberculosis. In: Rom WN, Garay SM, editors. Tuberculosis. Philadelphia: Lippincott Williams & Wilkins; 2004. pp. 427–444.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
