

Middle frontal horizontal partial laryngectomy (MFHPL): a treatment for stage T1b squamous cell carcinoma of the glottic larynx involving anterior vocal commissure
- PMID: 23326350
- PMCID: PMC3541376
- DOI: 10.1371/journal.pone.0052723
Middle frontal horizontal partial laryngectomy (MFHPL): a treatment for stage T1b squamous cell carcinoma of the glottic larynx involving anterior vocal commissure
Abstract
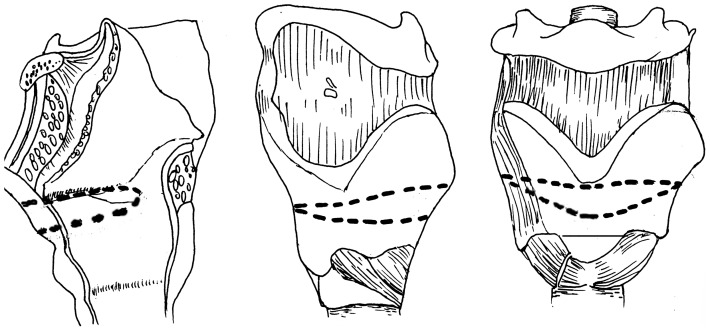
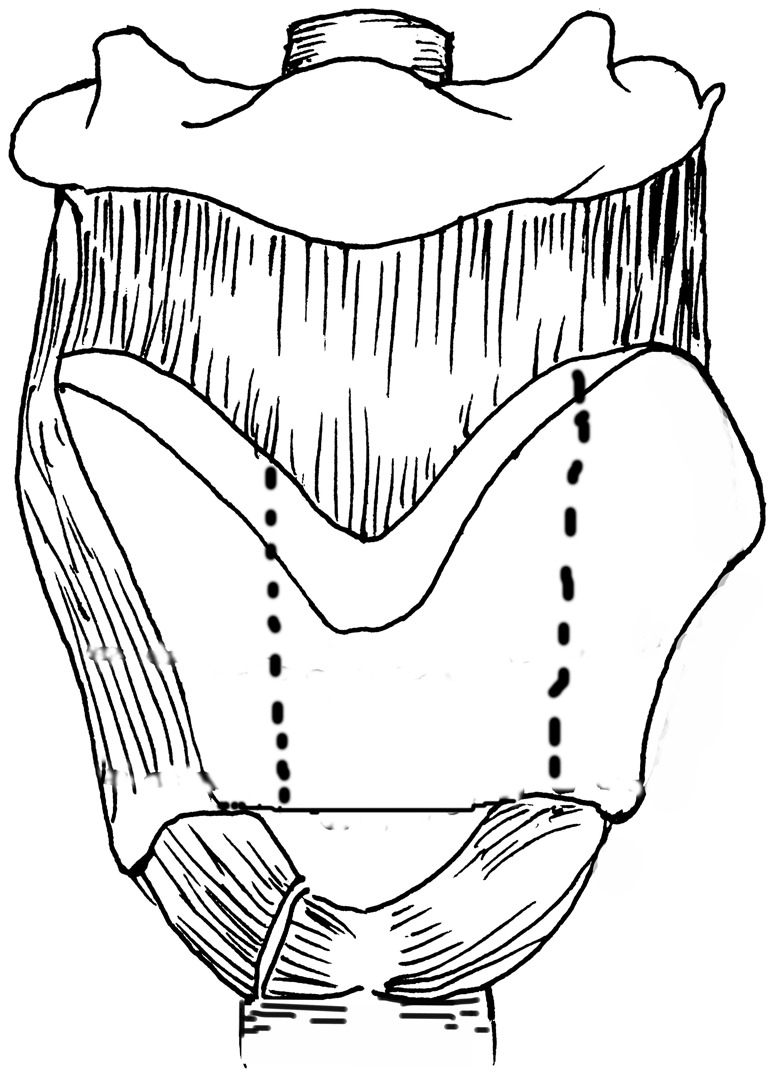
Objective: The therapeutic effect of middle frontal horizontal partial laryngectomy (MFHPL) in treating stage T1b squamous cell carcinoma of the glottic larynx involving anterior vocal commissure (AVC) was compared with that of the anterior frontolateral vertical partial laryngectomy (AFVPL). The feasibility and practical significance of MFHPL in clinical application was discussed in the present study.
Methods: From January 1996 to January 2010, a total of 65 patients diagnosed with stage T1bN0M0 glottic laryngeal cancer were treated with MFHPL or AFVPL. The postoperative complications, glottic reconstruction, recurrence rate, voice quality and survival rates were evaluated and compared between two treatments.
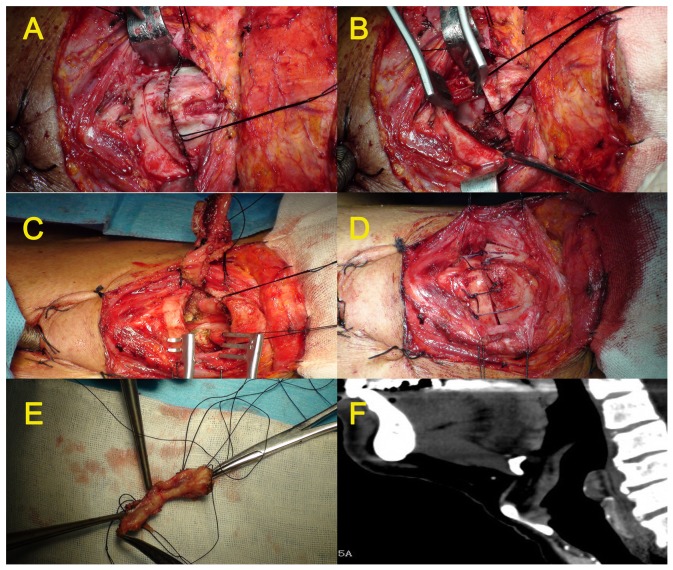
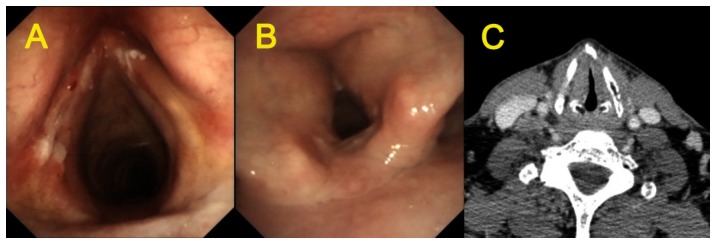
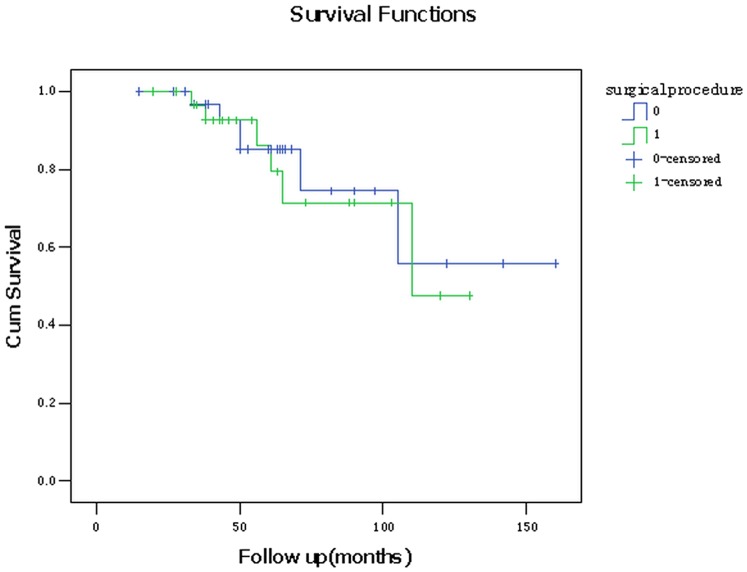
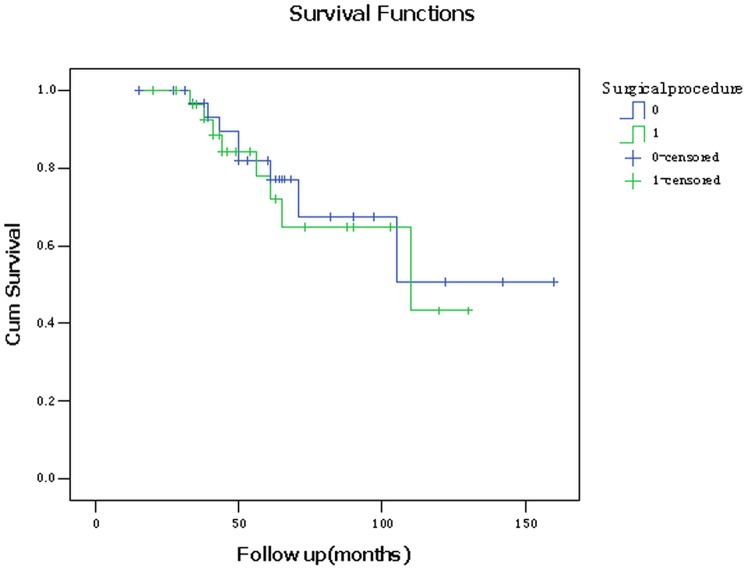
Results: AFVPL and MFHPL were performed in 34 and 31 patients, respectively. Flexible fiberoptic laryngoscopy revealed that in the MFHPL-treated patients the reconstructed glottis was spacious and symmetric. In contrast, AFVPL treatment resulted in irregular glottic area with poor symmetry and tubular glottis. The incidence of postoperative laryngeal stenosis significantly differed between the MFHPL- and AFVPL-treated groups (P = 0.025). No significant difference was detected in the 3- and 5-year overall- or tumor-free survival rates between two treatments. The Voice Handicap Index (VHI) and maximum phonation time (MPT) after surgery were 51.0±12.99 and 12.42±3.44 sec in the AFVPL-treated group; while in the MFHPL-treated patients they were 31.81±7.48 and 7.65±1.98 sec, respectively. Both differences in VHI (P = 0.012) and MPT (P = 0.024) were significant between two treatments.
Conclusions: MFHPL was comparable to AFVPL with respect to postoperative complications, recurrence rate and survival rates, but possessed advantages over AFVPL in terms of the incidence of laryngeal stenosis and voice quality. Our study indicated that MFHPL has a potential value in clinical practice of treating stage T1b squamous cell carcinoma of the glottic larynx involving AVC.
Conflict of interest statement
Figures
Similar articles
-
Outcomes of frontolateral vertical partial laryngectomy in T1b glottic carcinomas.Acta Otolaryngol. 2021 Jan;141(1):99-105. doi: 10.1080/00016489.2020.1816659. Epub 2020 Sep 17. Acta Otolaryngol. 2021. PMID: 32940106
-
Supracricoid partial laryngectomy with cricothyroidopexy: a treatment for anterior vocal commissure laryngeal squamous carcinoma.Head Neck. 2013 Mar;35(3):311-5. doi: 10.1002/hed.22965. Epub 2012 Feb 24. Head Neck. 2013. PMID: 22367764
-
Clinical outcome of window partial laryngectomy for stage T2-3 glottic laryngeal carcinoma.J Voice. 2011 Jan;25(1):124-8. doi: 10.1016/j.jvoice.2009.07.001. Epub 2010 Feb 19. J Voice. 2011. PMID: 20171837
-
Laser Microsurgery Versus Radiotherapy Versus Open Partial Laryngectomy for T2 Laryngeal Carcinoma: A Systematic Review of Oncological Outcomes.Ear Nose Throat J. 2021 Feb;100(1_suppl):51S-58S. doi: 10.1177/0145561320928198. Epub 2020 Jun 8. Ear Nose Throat J. 2021. PMID: 32511005
-
Partial laryngectomy after irradiation failure.Otolaryngol Head Neck Surg. 2003 Feb;128(2):200-9. doi: 10.1067/mhn.2003.63. Otolaryngol Head Neck Surg. 2003. PMID: 12601315 Review.
Cited by
-
Tucker's Reconstructive Laryngectomy: Indications and Functional Outcomes.Iran J Otorhinolaryngol. 2025;37(1):3-9. doi: 10.22038/ijorl.2024.78978.3660. Iran J Otorhinolaryngol. 2025. PMID: 39850228 Free PMC article.
-
Comment to the article "Open partial horizontal laryngectomies: a proposal for classification by the working committee on nomenclature of the European Laryngological Society" by G. Succo et al.Eur Arch Otorhinolaryngol. 2015 Apr;272(4):1041-1042. doi: 10.1007/s00405-014-3222-0. Epub 2014 Aug 8. Eur Arch Otorhinolaryngol. 2015. PMID: 25104060 Free PMC article. No abstract available.
-
Adverse histopathological findings in glottic cancer with anterior commissure involvement.Eur Arch Otorhinolaryngol. 2015 Aug;272(8):1973-81. doi: 10.1007/s00405-015-3594-9. Epub 2015 Mar 21. Eur Arch Otorhinolaryngol. 2015. PMID: 25794542
-
Transoral laser microsurgery for T1b glottic cancer: review of 51 cases.Eur Arch Otorhinolaryngol. 2017 Apr;274(4):1997-2004. doi: 10.1007/s00405-016-4432-4. Epub 2016 Dec 27. Eur Arch Otorhinolaryngol. 2017. PMID: 28028607
-
Therapeutic modalities and oncologic outcomes in the treatment of T1b glottic squamous cell carcinoma: a systematic review.Eur Arch Otorhinolaryngol. 2017 Dec;274(12):4091-4102. doi: 10.1007/s00405-017-4736-z. Epub 2017 Sep 19. Eur Arch Otorhinolaryngol. 2017. PMID: 28929221
References
-
- Bradley PJ, Rinaldo A, Suarez C, Shaha AR, Leemans CR, et al. (2006) Primary treatment of the anterior vocal commissure squamous carcinoma. Eur Arch Otorhinolaryngo 263: 879–888. - PubMed
-
- Herranz J, Gavilan J, Vazquez-Barros JC (2007) Carcinoma of the anterior commissure. Acta Otorrinolaringol Esp 58: 367–370. - PubMed
-
- Silver CE, Beitler JJ, Shaha AR, Rinaldo A, Ferlito A (2009) Current trends in initial management of laryngeal cancer: the declining use of open surgery. Eur Arch Otorhinolaryngol 266: 1333–1352. - PubMed
-
- Chone CT, Yonehara E, Martins JE, Altemani A, Crespo AN (2007) Importance of anterior commissure in recurrence of early glottic cancer after laser endoscopic resection. Arch Otolaryngol Head Neck Surg 133: 882–887. - PubMed
-
- Ganly I, Patel SG, Matsuo J, Singh B, Kraus DH, et al. (2009) Analysis of postoperative complications of open partial laryngectomy. Head Neck 31: 338–345. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
