

Psychoacoustic tinnitus loudness and tinnitus-related distress show different associations with oscillatory brain activity
- PMID: 23326394
- PMCID: PMC3542397
- DOI: 10.1371/journal.pone.0053180
Psychoacoustic tinnitus loudness and tinnitus-related distress show different associations with oscillatory brain activity
Abstract
Background: The phantom auditory perception of subjective tinnitus is associated with aberrant brain activity as evidenced by magneto- and electroencephalographic studies. We tested the hypotheses (1) that psychoacoustically measured tinnitus loudness is related to gamma oscillatory band power, and (2) that tinnitus loudness and tinnitus-related distress are related to distinct brain activity patterns as suggested by the distinction between loudness and distress experienced by tinnitus patients. Furthermore, we explored (3) how hearing impairment, minimum masking level, and (4) psychological comorbidities are related to spontaneous oscillatory brain activity in tinnitus patients.
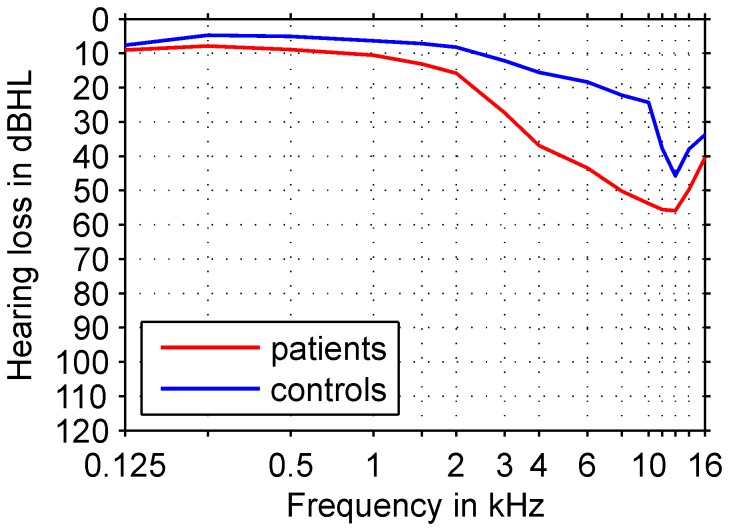
Methods and findings: Resting state oscillatory brain activity recorded electroencephalographically from 46 male tinnitus patients showed a positive correlation between gamma band oscillations and psychoacoustic tinnitus loudness determined with the reconstructed tinnitus sound, but not with the other psychoacoustic loudness measures that were used. Tinnitus-related distress did also correlate with delta band activity, but at electrode positions different from those associated with tinnitus loudness. Furthermore, highly distressed tinnitus patients exhibited a higher level of theta band activity. Moreover, mean hearing loss between 0.125 kHz and 16 kHz was associated with a decrease in gamma activity, whereas minimum masking levels correlated positively with delta band power. In contrast, psychological comorbidities did not express significant correlations with oscillatory brain activity.
Conclusion: Different clinically relevant tinnitus characteristics show distinctive associations with spontaneous brain oscillatory power. Results support hypothesis (1), but exclusively for the tinnitus loudness derived from matching to the reconstructed tinnitus sound. This suggests to preferably use the reconstructed tinnitus spectrum to determine psychoacoustic tinnitus loudness. Results also support hypothesis (2). Moreover, hearing loss and minimum masking level correlate with oscillatory power in distinctive frequency bands. The lack of an association between psychological comorbidities and oscillatory power may be attributed to the overall low level of mental health problems in the present sample.
Conflict of interest statement
Figures
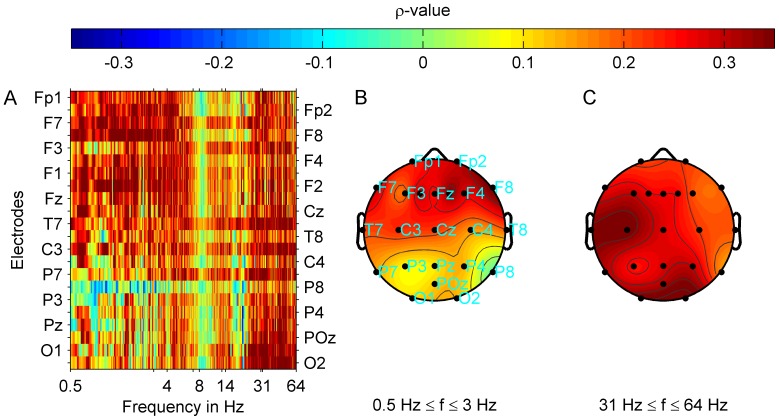
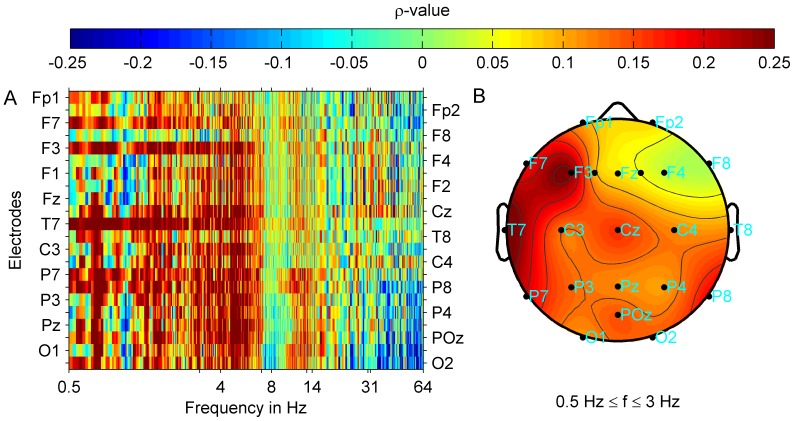
 ) at each electrode and frequency point is shown. Plots (B) and (C) show correlation maps corresponding to (A) with averaged correlation strength (
) at each electrode and frequency point is shown. Plots (B) and (C) show correlation maps corresponding to (A) with averaged correlation strength ( ) topographies for the tinnitus loudness
) topographies for the tinnitus loudness  and delta (B) or gamma (C) oscillatory power. Correlation strength for delta band power and tinnitus loudness was highest in the frontal half of the brain and lowest at posterior locations. For the correlation between gamma band power and tinnitus loudness the distribution of correlation strength across electrode positions was more uniform. Highest correlation strength was reached at the left temporal and right occipital electrode positions. After FDR correction (FDR 0.05:
and delta (B) or gamma (C) oscillatory power. Correlation strength for delta band power and tinnitus loudness was highest in the frontal half of the brain and lowest at posterior locations. For the correlation between gamma band power and tinnitus loudness the distribution of correlation strength across electrode positions was more uniform. Highest correlation strength was reached at the left temporal and right occipital electrode positions. After FDR correction (FDR 0.05:  ) correlations remained significant at all electrode positions except for T8 and P8 locations for the gamma band, whereas significant correlations in the delta band were attained at the fronto-central locations Fp2, F1, Fz, F2, F4, F8, C3, Cz, and at P7.
) correlations remained significant at all electrode positions except for T8 and P8 locations for the gamma band, whereas significant correlations in the delta band were attained at the fronto-central locations Fp2, F1, Fz, F2, F4, F8, C3, Cz, and at P7.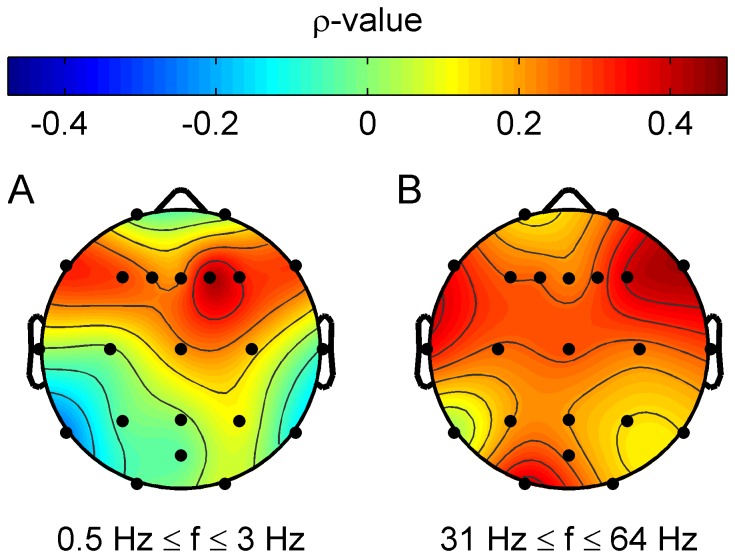
 ) at each electrode and frequency point is shown. Plot (B) shows the correlation map with averaged correlation strength (
) at each electrode and frequency point is shown. Plot (B) shows the correlation map with averaged correlation strength ( ) topographies between MML and delta oscillatory power. After FDR correction, correlations at the F8 and T8 electrode position remained significant (FDR 0.05:
) topographies between MML and delta oscillatory power. After FDR correction, correlations at the F8 and T8 electrode position remained significant (FDR 0.05:  ).
).
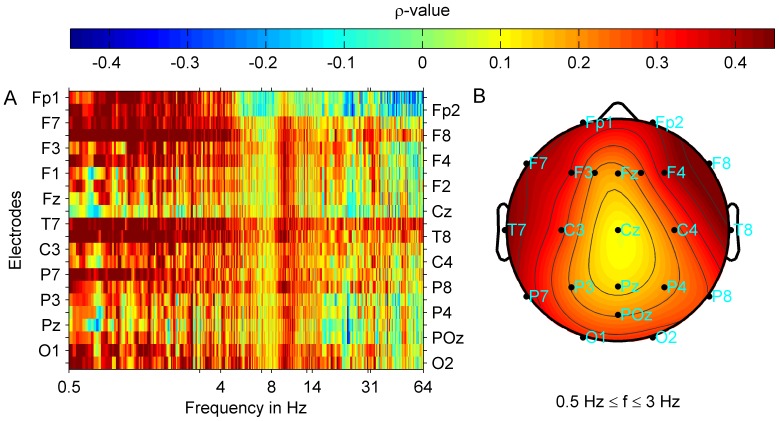
 ) at each electrode and frequency point is shown. Plot (B) shows the correlation map with averaged correlation strength (
) at each electrode and frequency point is shown. Plot (B) shows the correlation map with averaged correlation strength ( ) topographies between tinnitus-related distress and delta band power. Irrespective of tinnitus laterality, correlation strength is most pronounced at frontal and temporal locations of the left hemisphere. After FDR correction (FDR 0.05) correlations did not remain significant.
) topographies between tinnitus-related distress and delta band power. Irrespective of tinnitus laterality, correlation strength is most pronounced at frontal and temporal locations of the left hemisphere. After FDR correction (FDR 0.05) correlations did not remain significant.Similar articles
-
Neuromagnetic indicators of tinnitus and tinnitus masking in patients with and without hearing loss.J Assoc Res Otolaryngol. 2012 Oct;13(5):715-31. doi: 10.1007/s10162-012-0340-5. Epub 2012 Jul 12. J Assoc Res Otolaryngol. 2012. PMID: 22791191 Free PMC article.
-
Relationship Between Tinnitus Loudness Measure by Visual Analogue Scale and Psychoacoustic Matching of Tinnitus Loudness.Otol Neurotol. 2019 Jan;40(1):16-21. doi: 10.1097/MAO.0000000000002070. Otol Neurotol. 2019. PMID: 30540695
-
The neural correlates of subjectively perceived and passively matched loudness perception in auditory phantom perception.Brain Behav. 2015 May;5(5):e00331. doi: 10.1002/brb3.331. Epub 2015 Mar 19. Brain Behav. 2015. PMID: 25874164 Free PMC article.
-
A Pilot Study to Evaluate a Residual Inhibition Technique in Hearing Aids for Suppression of Tinnitus.Semin Hear. 2023 Jun 28;45(1):123-140. doi: 10.1055/s-0043-1770153. eCollection 2024 Feb. Semin Hear. 2023. PMID: 38370522 Free PMC article. Review.
-
Psychoacoustic measures of tinnitus.J Am Acad Audiol. 2000 Mar;11(3):138-55. J Am Acad Audiol. 2000. PMID: 10755810 Review.
Cited by
-
Changes in Speech-Related Brain Activity During Adaptation to Electro-Acoustic Hearing.Front Neurol. 2020 Mar 31;11:161. doi: 10.3389/fneur.2020.00161. eCollection 2020. Front Neurol. 2020. PMID: 32300327 Free PMC article.
-
Reducing Tinnitus via Inhibitory Influence of the Sensorimotor System on Auditory Cortical Activity.J Neurosci. 2025 Apr 23;45(17):e0581242025. doi: 10.1523/JNEUROSCI.0581-24.2025. J Neurosci. 2025. PMID: 39952670
-
Tinnitus, sound intolerance, and mental health: the role of long-term occupational noise exposure.Eur Arch Otorhinolaryngol. 2022 Nov;279(11):5161-5170. doi: 10.1007/s00405-022-07362-2. Epub 2022 Mar 31. Eur Arch Otorhinolaryngol. 2022. PMID: 35359185
-
Cochlear Implant and Hearing Aid: Objective Measures of Binaural Benefit.Front Neurosci. 2020 Dec 14;14:586119. doi: 10.3389/fnins.2020.586119. eCollection 2020. Front Neurosci. 2020. PMID: 33381008 Free PMC article.
-
Psychoacoustic classification of persistent tinnitus.Braz J Otorhinolaryngol. 2018 Sep-Oct;84(5):583-590. doi: 10.1016/j.bjorl.2017.07.005. Epub 2017 Aug 1. Braz J Otorhinolaryngol. 2018. PMID: 28826945 Free PMC article.
References
-
- Sindhusake D, Golding M, Newall P, Rubin G, Jakobsen K, et al. (2003) Risk factors for tinnitus in a population of older adults: the blue mountains hearing study. Ear Hear 24: 501. - PubMed
-
- Weisz N, Dohrmann K, Elbert T (2007) The relevance of spontaneous activity for the coding of the tinnitus sensation. Prog Brain Res 166: 61–70. - PubMed
-
- Rosenhall U (2003) The influence of ageing on noise-induced hearing loss. Noise Health 5: 47–53. - PubMed
-
- Krog NH, Engdahla B, Tambs K (2010) The association between tinnitus and mental health in a general population sample: results from the hunt study. J Psychosom Res 69: 289–298. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
