

MRSA nasal carriage patterns and the subsequent risk of conversion between patterns, infection, and death
- PMID: 23326483
- PMCID: PMC3542362
- DOI: 10.1371/journal.pone.0053674
MRSA nasal carriage patterns and the subsequent risk of conversion between patterns, infection, and death
Abstract
Background: Patterns of methicillin-resistant S. aureus (MRSA) nasal carriage over time and across the continuum of care settings are poorly characterized. Knowledge of prevalence rates and outcomes associated with MRSA nasal carriage patterns could help direct infection prevention strategies. The VA integrated health-care system and active surveillance program provides an opportunity to delineate nasal carriage patterns and associated outcomes of death, infection, and conversion in carriage.
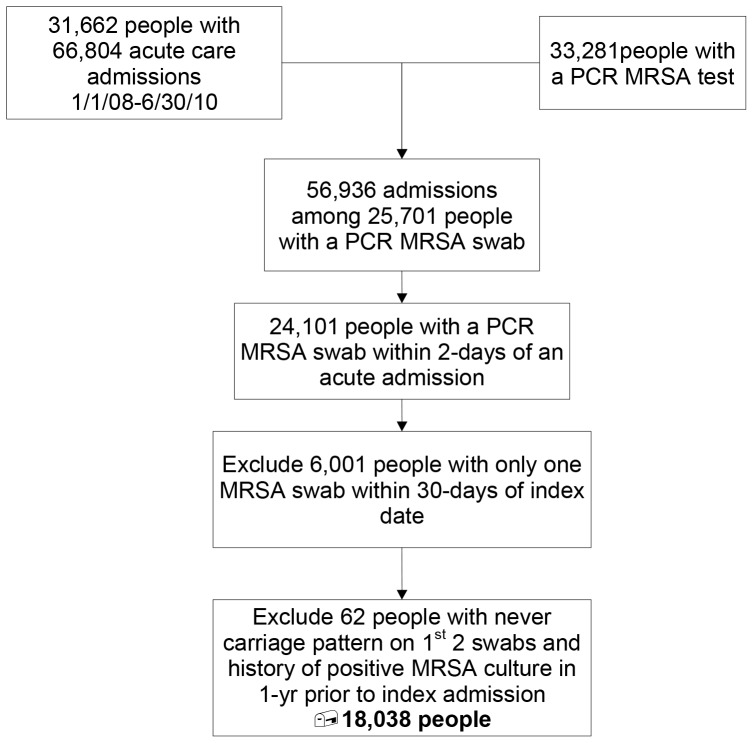
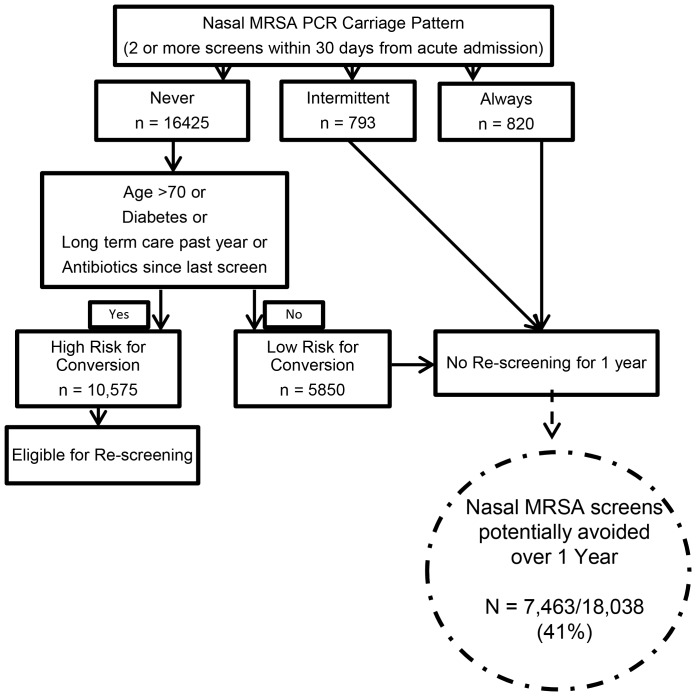
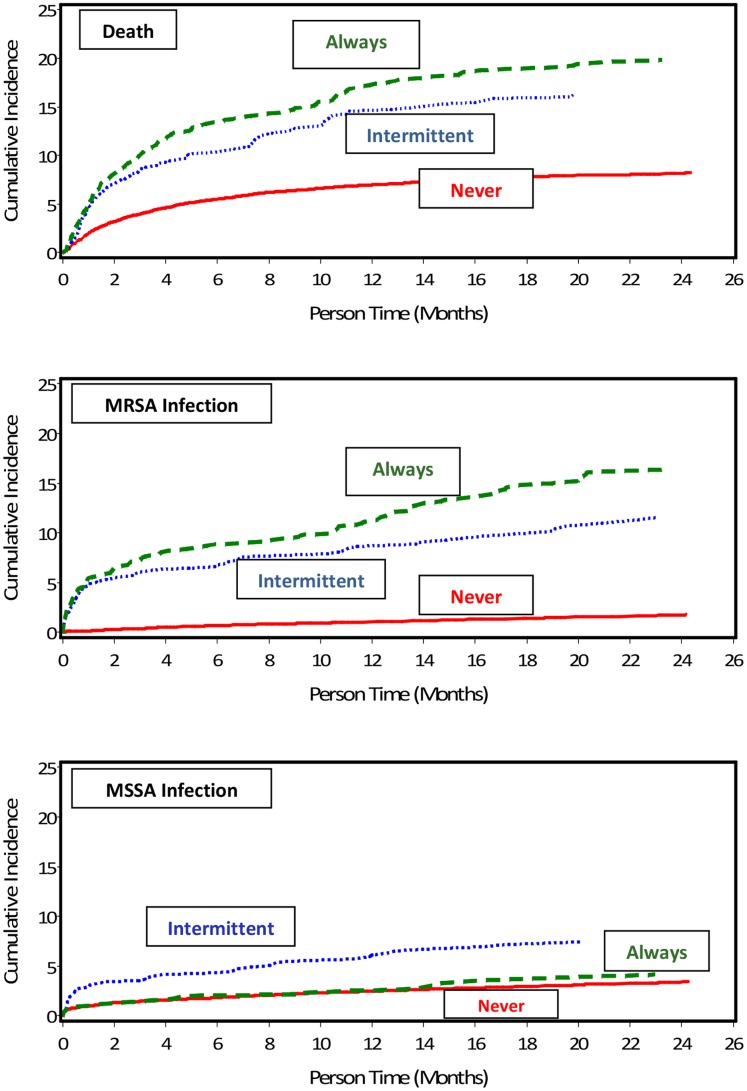
Methods/findings: We conducted a retrospective cohort study including all patients admitted to 5 acute care VA hospitals between 2008-2010 who had nasal MRSA PCR testing within 48 hours of admission and repeat testing within 30 days. The PCR results were used to define a baseline nasal carriage pattern of never, intermittently, or always colonized at 30 days from admission. Follow-up was up to two years and included acute, long-term, and outpatient care visits. Among 18,038 patients, 91.1%, 4.4%, and 4.6% were never, intermittently, or always colonized at the 30-day baseline. Compared to non-colonized patients, those who were persistently colonized had an increased risk of death (HR 2.58; 95% CI 2.18;3.05) and MRSA infection (HR 10.89; 95% CI 8.6;13.7). Being in the non-colonized group at 30 days had a predictive value of 87% for being non-colonized at 1 year. Conversion to MRSA colonized at 6 months occurred in 11.8% of initially non-colonized patients. Age >70 years, long-term care, antibiotic exposure, and diabetes identified >95% of converters.
Conclusions: The vast majority of patients are not nasally colonized with MRSA at 30 days from acute hospital admission. Conversion from non-carriage is infrequent and can be risk-stratified. A positive carriage pattern is strongly associated with infection and death. Active surveillance programs in the year following carriage pattern designation could be tailored to focus on non-colonized patients who are at high risk for conversion, reducing universal screening burden.
Conflict of interest statement
Figures
References
-
- Wertheim HF, Melles DC, Vos MC, van Leeuwen W, van Belkum A, et al. (2005) The role of nasal carriage in Staphylococcus aureus infections. Lancet Infect Dis 5: 751–762. - PubMed
-
- Huang SS, Platt R (2003) Risk of methicillin-resistant Staphylococcus aureus infection after previous infection or colonization. Clin Infect Dis 36: 281–285. - PubMed
-
- Avery TR, Kleinman KP, Klompas M, Aschengrau A, Huang SS (2012) Inclusion of 30-Day Postdischarge Detection Triples the Incidence of Hospital-Onset Methicillin-Resistant Staphylococcus aureus. Infect Control Hosp Epidemiol 33: 114–121. - PubMed
-
- Davis KA, Stewart JJ, Crouch HK, Florez CE, Hospenthal DR (2004) Methicillin-resistant Staphylococcus aureus (MRSA) nares colonization at hospital admission and its effect on subsequent MRSA infection. Clin Infect Dis 39: 776–782. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
