

Malaria and fetal growth alterations in the 3(rd) trimester of pregnancy: a longitudinal ultrasound study
- PMID: 23326508
- PMCID: PMC3543265
- DOI: 10.1371/journal.pone.0053794
Malaria and fetal growth alterations in the 3(rd) trimester of pregnancy: a longitudinal ultrasound study
Abstract
Background: Pregnancy associated malaria is associated with decreased birth weight, but in-utero evaluation of fetal growth alterations is rarely performed. The objective of this study was to investigate malaria induced changes in fetal growth during the 3(rd) trimester using trans-abdominal ultrasound.
Methods: An observational study of 876 pregnant women (398 primi- and secundigravidae and 478 multigravidae) was conducted in Tanzania. Fetal growth was monitored with ultrasound and screening for malaria was performed regularly. Birth weight and fetal weight were converted to z-scores, and fetal growth evaluated as fetal weight gain from the 26th week of pregnancy.
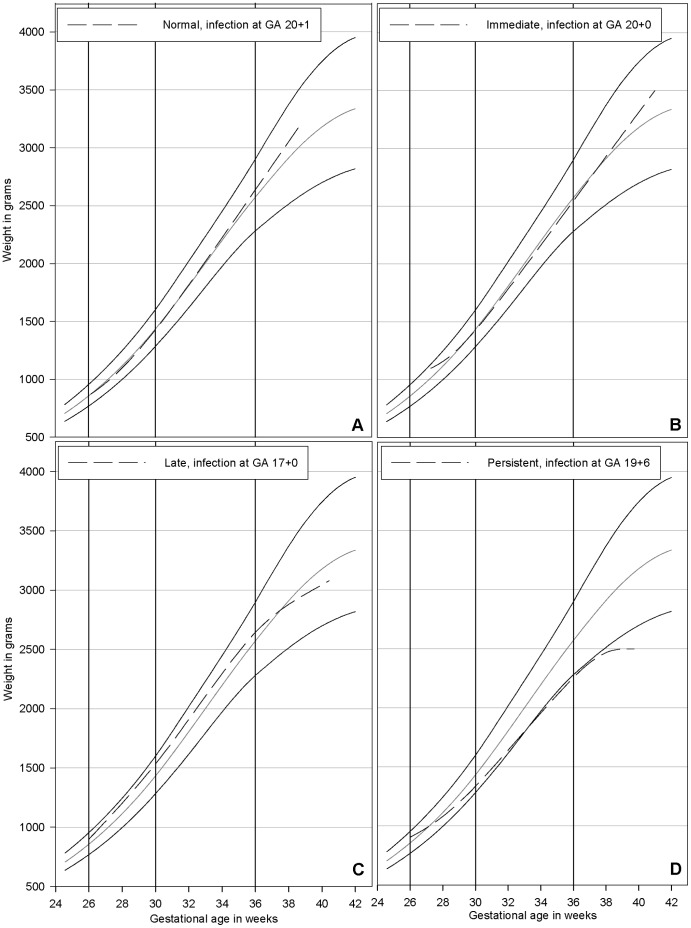
Results: Malaria infection only affected birth weight and fetal growth among primi- and secundigravid women. Forty-eight of the 398 primi- and secundigravid women had malaria during pregnancy causing a reduction in the newborns z-score of -0.50 (95% CI: -0.86, -0.13, P = 0.008, multiple linear regression). Fifty-eight percent (28/48) of the primi- and secundigravidae had malaria in the first half of pregnancy, but an effect on fetal growth was observed in the 3(rd) trimester with an OR of 4.89 for the fetal growth rate belonging to the lowest 25% in the population (95%CI: 2.03-11.79, P<0.001, multiple logistic regression). At an individual level, among the primi- and secundigravidae, 27% experienced alterations of fetal growth immediately after exposure but only for a short interval, 27% only late in pregnancy, 16.2% persistently from exposure until the end of pregnancy, and 29.7% had no alterations of fetal growth.
Conclusions: The effect of malaria infections was observed during the 3(rd) trimester, despite infections occurring much earlier in pregnancy, and different mechanisms might operate leading to different patterns of growth alterations. This study highlights the need for protection against malaria throughout pregnancy and the recognition that observed changes in fetal growth might be a consequence of an infection much earlier in pregnancy.
Conflict of interest statement
Figures
References
-
- Shulman CE, Marshall T, Dorman EK, Bulmer JN, Cutts F, et al. (2001) Malaria in pregnancy: adverse effects on haemoglobin levels and birthweight in primigravidae and multigravidae. Trop Med Int Health 6: 770–778. - PubMed
-
- Sullivan AD, Nyirenda T, Cullinan T, Taylor T, Harlow SD, et al. (1999) Malaria infection during pregnancy: intrauterine growth retardation and preterm delivery in Malawi. J Infect Dis 179: 1580–1583. - PubMed
-
- Steketee RW, Wirima JJ, Hightower AW, Slutsker L, Heymann DL, et al. (1996) The effect of malaria and malaria prevention in pregnancy on offspring birthweight, prematurity, and intrauterine growth retardation in rural Malawi. Am J Trop Med Hyg 55: 33–41. - PubMed
-
- Meuris S, Piko BB, Eerens P, Vanbellinghen AM, Dramaix M, et al. (1993) Gestational malaria: assessment of its consequences on fetal growth. Am J Trop Med Hyg 48: 603–609. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
