

Haloperidol prophylaxis in critically ill patients with a high risk for delirium
- PMID: 23327295
- PMCID: PMC4056261
- DOI: 10.1186/cc11933
Haloperidol prophylaxis in critically ill patients with a high risk for delirium
Abstract
Introduction: Delirium is associated with increased morbidity and mortality. We implemented a delirium prevention policy in intensive care unit (ICU) patients with a high risk of developing delirium, and evaluated if our policy resulted in quality improvement of relevant delirium outcome measures.
Methods: This study was a before/after evaluation of a delirium prevention project using prophylactic treatment with haloperidol. Patients with a predicted risk for delirium of ≥ 50%, or with a history of alcohol abuse or dementia, were identified. According to the prevention protocol these patients received haloperidol 1 mg/8 h. Evaluation was primarily focused on delirium incidence, delirium free days without coma and 28-day mortality. Results of prophylactic treatment were compared with a historical control group and a contemporary group that did not receive haloperidol prophylaxis mainly due to non-compliance to the protocol mostly during the implementation phase.
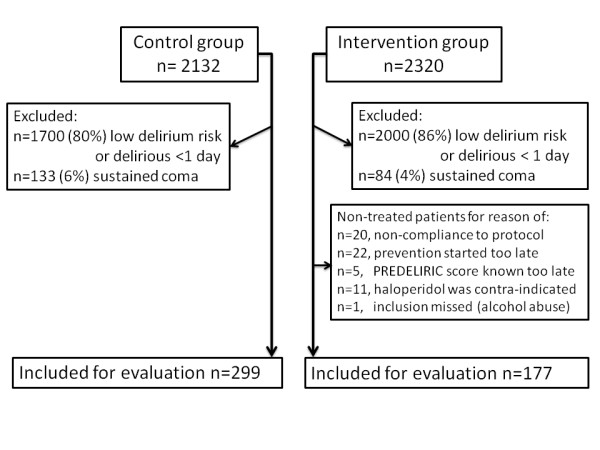
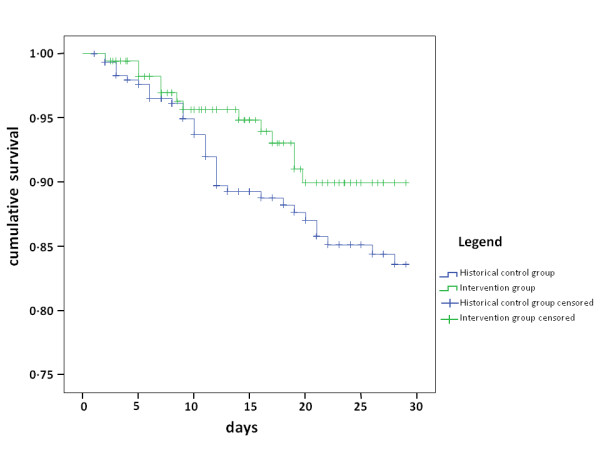
Results: In 12 months, 177 patients received haloperidol prophylaxis. Except for sepsis, patient characteristics were comparable between the prevention and the historical (n = 299) groups. Predicted chance to develop delirium was 75 ± 19% and 73 ± 22%, respectively. Haloperidol prophylaxis resulted in a lower delirium incidence (65% vs. 75%, P = 0.01), and more delirium-free-days (median 20 days (IQR 8 to 27) vs. median 13 days (3 to 27), P = 0.003) in the intervention group compared to the control group. Cox-regression analysis adjusted for sepsis showed a hazard rate of 0.80 (95% confidence interval 0.66 to 0.98) for 28-day mortality. Beneficial effects of haloperidol appeared most pronounced in the patients with the highest risk for delirium. Furthermore, haloperidol prophylaxis resulted in less ICU re-admissions (11% vs. 18%, P = 0.03) and unplanned removal of tubes/lines (12% vs. 19%, P = 0.02). Haloperidol was stopped in 12 patients because of QTc-time prolongation (n = 9), renal failure (n = 1) or suspected neurological side-effects (n = 2). No other side-effects were reported. Patients who were not treated during the intervention period (n = 59) showed similar results compared to the untreated historical control group.
Conclusions: Our evaluation study suggests that prophylactic treatment with low dose haloperidol in critically ill patients with a high risk for delirium probably has beneficial effects. These results warrant confirmation in a randomized controlled trial.
Trial registration: clinicaltrial.gov Identifier: NCT01187667.
Figures
References
-
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) 4. Washington, DC: American Psychiatric Association; 1994.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
