

Scoring radiographic progression in ankylosing spondylitis: should we use the modified Stoke Ankylosing Spondylitis Spine Score (mSASSS) or the Radiographic Ankylosing Spondylitis Spinal Score (RASSS)?
- PMID: 23327723
- PMCID: PMC3672818
- DOI: 10.1186/ar4144
Scoring radiographic progression in ankylosing spondylitis: should we use the modified Stoke Ankylosing Spondylitis Spine Score (mSASSS) or the Radiographic Ankylosing Spondylitis Spinal Score (RASSS)?
Abstract
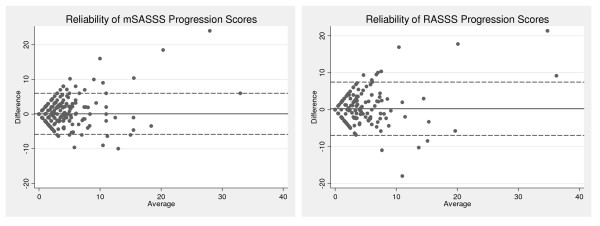
Introduction: Radiographic damage is one of the core outcomes in axial SpA and is usually assessed with the modified Stoke Ankylosing Spondylitis (AS) Spine Score (mSASSS). Alternatively, the Radiographic AS Spinal Score (RASSS) is proposed, which includes the lower thoracic vertebrae, under the hypothesis that most progression occurs in these segments. We aimed to compare the mSASSS and RASSS with regard to performance.
Methods: Two-yearly spinal radiographs from patients followed in the Outcome in AS International Study (OASIS) were used (scored independently by two readers). A total of 195 patients had at least one radiograph (12-year follow-up) to be included. We assessed the accessibility of vertebral corners (VCs) for scoring, as well as status and 2-year progression scores of both scoring methods. To assess the potential additional value of including the thoracic segment in the score, the relative contribution (in %) to the 2-year total RASSS progression of each spinal segment (cervical, thoracic and lumbar) was determined, and compared to the expected contribution, under the assumption that a balanced segmental progression would occur, proportional to the number of sites per segment.
Results: The mSASSS could be scored in a total of 809 radiographs and the RASSS in 78% of these. In 58% of the latter, the score was based on one to two available thoracic VCs scores, and the remaining two to three were imputed because they were missing. There were 520 two-year mSASSS intervals available, and in 63% of them RASSS progression could be assessed. The mean (SD) 2-year interval progression score (330 intervals) was 2.0 (3.6) for the mSASSS and 2.4 (4.4) for the RASSS, yielding a similar effect size (mSASSS 0.57 and RASSS 0.55). Exclusive progression of the thoracic segment occurred in only 5% of the cases. There was no significant difference between the observed (14%) and expected (16%) contribution to progression of the thoracic segment (P=0.70).
Conclusions: The determination of RASSS for radiographic damage of the spine is frequently impossible or strongly influenced by non-contributory imputation. In comparison to the mSASSS, the contribution of thoracic VCs in the RASSS method is negligible, and does not justify the additional scoring efforts.
Figures
Similar articles
-
Development of a radiographic scoring tool for ankylosing spondylitis only based on bone formation: addition of the thoracic spine improves sensitivity to change.Arthritis Rheum. 2009 Jun 15;61(6):764-71. doi: 10.1002/art.24425. Arthritis Rheum. 2009. PMID: 19479705
-
Which scoring method depicts spinal radiographic damage in early axial spondyloarthritis best? Five-year results from the DESIR cohort.Rheumatology (Oxford). 2018 Nov 1;57(11):1991-2000. doi: 10.1093/rheumatology/key185. Rheumatology (Oxford). 2018. PMID: 30053219
-
Incorporation of the anteroposterior lumbar radiographs in the modified Stoke Ankylosing Spondylitis Spine Score improves detection of radiographic spinal progression in axial spondyloarthritis.Arthritis Res Ther. 2019 May 24;21(1):126. doi: 10.1186/s13075-019-1913-z. Arthritis Res Ther. 2019. PMID: 31126334 Free PMC article.
-
Modified stoke ankylosing spondylitis spinal score as an outcome measure to assess the impact of treatment on structural progression in ankylosing spondylitis.Rheumatology (Oxford). 2019 Mar 1;58(3):388-400. doi: 10.1093/rheumatology/key128. Rheumatology (Oxford). 2019. PMID: 29860356 Free PMC article. Review.
-
Effect of TNF-inhibitor therapy on spinal structural progression in ankylosing spondylitis patients: A systematic review and meta-analysis.Int J Rheum Dis. 2020 Jun;23(6):728-743. doi: 10.1111/1756-185X.13829. Epub 2020 May 17. Int J Rheum Dis. 2020. PMID: 32419337
Cited by
-
Evaluation of the change in structural radiographic sacroiliac joint damage after 2 years of etanercept therapy (EMBARK trial) in comparison to a contemporary control cohort (DESIR cohort) in recent onset axial spondyloarthritis.Ann Rheum Dis. 2018 Feb;77(2):221-227. doi: 10.1136/annrheumdis-2017-212008. Epub 2017 Sep 29. Ann Rheum Dis. 2018. PMID: 28970213 Free PMC article. Clinical Trial.
-
Limited radiographic progression and sustained reductions in MRI inflammation in patients with axial spondyloarthritis: 4-year imaging outcomes from the RAPID-axSpA phase III randomised trial.Ann Rheum Dis. 2018 May;77(5):699-705. doi: 10.1136/annrheumdis-2017-212377. Epub 2018 Jan 17. Ann Rheum Dis. 2018. PMID: 29343510 Free PMC article. Clinical Trial.
-
Spinal Radiographic Progression in Early Axial Spondyloarthritis: Five-Year Results From the DESIR Cohort.Arthritis Care Res (Hoboken). 2019 Dec;71(12):1678-1684. doi: 10.1002/acr.23796. Epub 2019 Nov 14. Arthritis Care Res (Hoboken). 2019. PMID: 30354022 Free PMC article.
-
Incorporating assessment of the cervical facet joints in the modified Stoke ankylosing spondylitis spine score is of additional value in the evaluation of spinal radiographic outcome in ankylosing spondylitis.Arthritis Res Ther. 2017 Apr 26;19(1):77. doi: 10.1186/s13075-017-1285-1. Arthritis Res Ther. 2017. PMID: 28441960 Free PMC article.
-
Sick leave and its predictors in ankylosing spondylitis: long-term results from the Outcome in Ankylosing Spondylitis International Study.RMD Open. 2018 Nov 27;4(2):e000766. doi: 10.1136/rmdopen-2018-000766. eCollection 2018. RMD Open. 2018. PMID: 30564453 Free PMC article.
References
-
- van der Heijde D, Calin A, Dougados M, Khan MA, van der Linden S, Bellamy N. Selection of instruments in the core set for DC-ART, SMARD, physical therapy, and clinical record keeping in ankylosing spondylitis. Progress report of the ASAS Working Group. Assessments in Ankylosing Spondylitis. J Rheumatol. 1999;26:951–954. - PubMed
-
- Wanders A, Landewe R, Dougados M, Mielants H, van der Linden S, van der Heijde D. Association between radiographic damage of the spine and spinal mobility for individual patients with ankylosing spondylitis: can assessment of spinal mobility be a proxy for radiographic evaluation? Ann Rheum Dis. 2005;64:988–994. doi: 10.1136/ard.2004.029728. - DOI - PMC - PubMed
-
- Zochling J, van der Heijde D, Burgos-Vargas R, Collantes E, Davis JC Jr, Dijkmans B, Dougados M, Geher P, Inman RD, Khan MA, Kvien TK, Leirisalo-Repo M, Olivieri I, Pavelka K, Sieper J, Stucki G, Sturrock RD, van der Linden S, Wendling D, Bohm H, van Royen BJ, Braun J. ASAS/EULAR recommendations for the management of ankylosing spondylitis. Ann Rheum Dis. 2006;65:442–452. doi: 10.1136/ard.2005.041137. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
