

Mechanisms of stroke after intracranial angioplasty and stenting in the SAMMPRIS trial
- PMID: 23328689
- PMCID: PMC3696348
- DOI: 10.1227/NEU.0b013e318286fdc8
Mechanisms of stroke after intracranial angioplasty and stenting in the SAMMPRIS trial
Abstract
Background: Enrollment in the stenting and aggressive medical management for the prevention of stroke in intracranial stenosis (SAMMPRIS) trial was halted owing to higher-than-expected 30-day stroke rates in the stenting arm. Improvement in periprocedural stroke rates from angioplasty and stenting for intracranial atherosclerotic disease (ICAD) requires an understanding of the mechanisms of these events.
Objective: To identify the types and mechanisms of periprocedural stroke after angioplasty and stenting for ICAD.
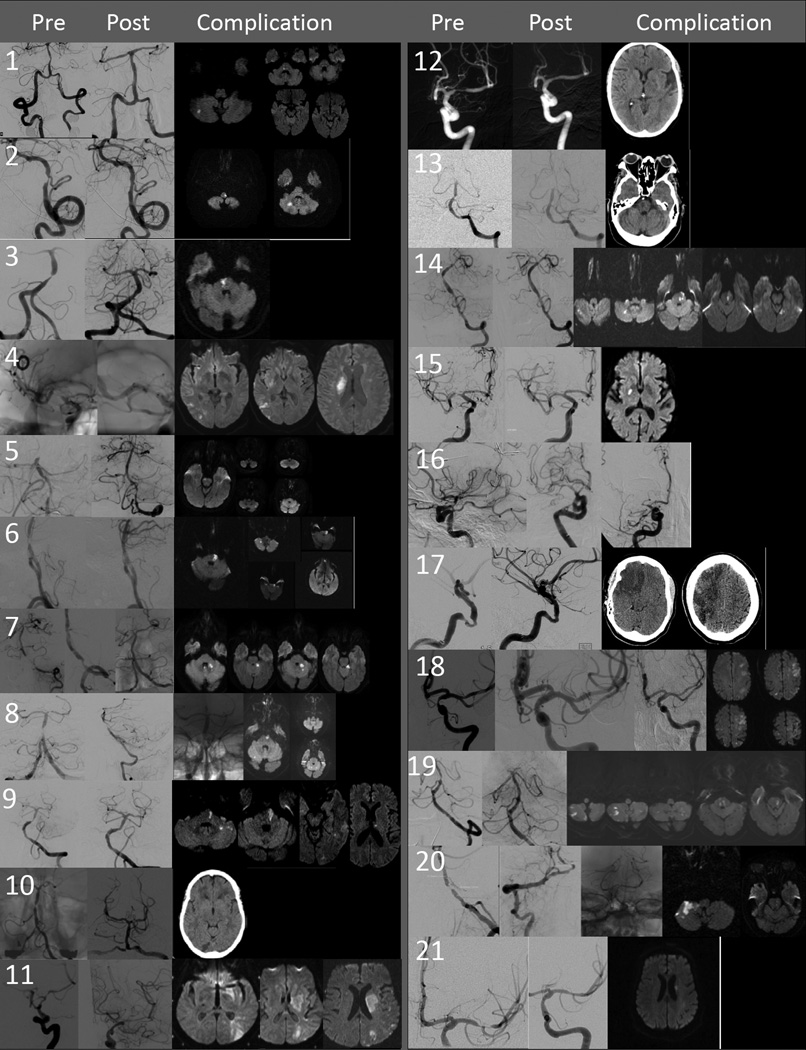
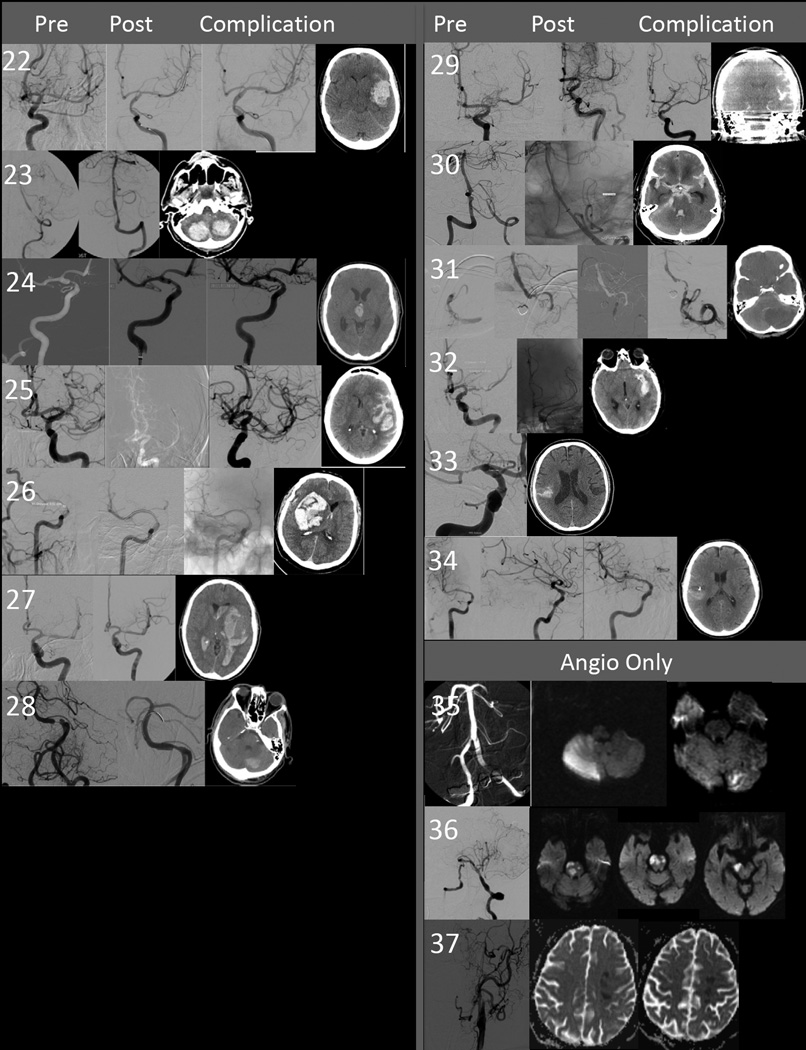
Methods: Patients who experienced a hemorrhagic or ischemic stroke or a cerebral infarct with temporary signs within 30 days of attempted angioplasty and stenting in SAMMPRIS were identified. Study records, including case report forms, procedure notes, and imaging were reviewed. Strokes were categorized as ischemic or hemorrhagic. Ischemic strokes were categorized as perforator territory, distal embolic, or delayed stent thrombosis. Hemorrhagic strokes were categorized as subarachnoid or intraparenchymal. Causes of hemorrhage (wire perforation, vessel rupture) were recorded.
Results: Three patients had an ischemic stroke after diagnostic angiography. Two of these strokes were unrelated to the procedure. Twenty-one patients had an ischemic stroke (n = 19) or cerebral infarct with temporary signs (n = 2) within 30 days of angioplasty and stenting. Most (n = 15) were perforator territory and many of these occurred after angiographically successful angioplasty and stenting of the basilar artery (n = 8). Six patients experienced a subarachnoid hemorrhage (3 from wire perforation) and 7 had a delayed intraparenchymal hemorrhage.
Conclusion: Efforts at reducing complications from angioplasty and stenting for ICAD must focus on reducing the risks of regional perforator infarction, delayed intraparenchymal hemorrhage, and wire perforation.
Figures
Comment in
-
Is there a contribution of anesthesia to the outcome of the SAMMPRIS trial?Neurosurgery. 2014 Feb;74(2):E234-5. doi: 10.1227/NEU.0000000000000211. Neurosurgery. 2014. PMID: 24141483 No abstract available.
-
In reply: Is there a contribution of anesthesia to the outcome of the SAMMPRIS trial?Neurosurgery. 2014 Feb;74(2):E235-6. doi: 10.1227/NEU.0000000000000227. Neurosurgery. 2014. PMID: 24149979 Free PMC article. No abstract available.
References
-
- Turan TN, Lynn MJ, Nizam A, et al. Rationale, Design, and Implementation of Aggressive Risk Factor Management in the Stenting and Aggressive Medical Management for Prevention of Recurrent Stroke in Intracranial Stenosis (SAMMPRIS) Trial. Circulation Cardiovascular quality and outcomes. 2012;5:e51–e60. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
- R01 NS036643/NS/NINDS NIH HHS/United States
- U01 NS058728/NS/NINDS NIH HHS/United States
- K23 NS069668/NS/NINDS NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- UL1RR029889/RR/NCRR NIH HHS/United States
- R01 NS051631/NS/NINDS NIH HHS/United States
- UL1 RR029882/RR/NCRR NIH HHS/United States
- UL1RR024131/RR/NCRR NIH HHS/United States
- UL1RR029890/RR/NCRR NIH HHS/United States
- 1K23 NS069668-01A1/NS/NINDS NIH HHS/United States
- TL1 RR029889/RR/NCRR NIH HHS/United States
- K24 NS050307/NS/NINDS NIH HHS/United States
- UG1 EY013287/EY/NEI NIH HHS/United States
- R01 NS051688/NS/NINDS NIH HHS/United States
- P50 55977/PHS HHS/United States
- P30 EY006360/EY/NEI NIH HHS/United States
- UL1 RR029890/RR/NCRR NIH HHS/United States
- U10 EY013287/EY/NEI NIH HHS/United States
- UL1RR029882/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
