

Unexpected clinical sequelae of Gitelman syndrome: hypertension in adulthood is common and females have higher potassium requirements
- PMID: 23328711
- PMCID: PMC3685308
- DOI: 10.1093/ndt/gfs600
Unexpected clinical sequelae of Gitelman syndrome: hypertension in adulthood is common and females have higher potassium requirements
Abstract
Background: Gitelman syndrome (GS) is a rare inherited disorder caused by mutations in SLC12A3, encoding the thiazide-sensitive transporter NCCT (sodium chloride co-transporter) in the distal tubule. It is characterized by renal potassium (K) and magnesium (Mg) wasting, relative hypotension and hypocalciuria. However, there is phenotypic variability and long-term studies are scarce.
Methods: We retrospectively assessed clinical and genetic characteristics, and electrolyte requirements, in a cohort of 36 patients with genetically proven GS.
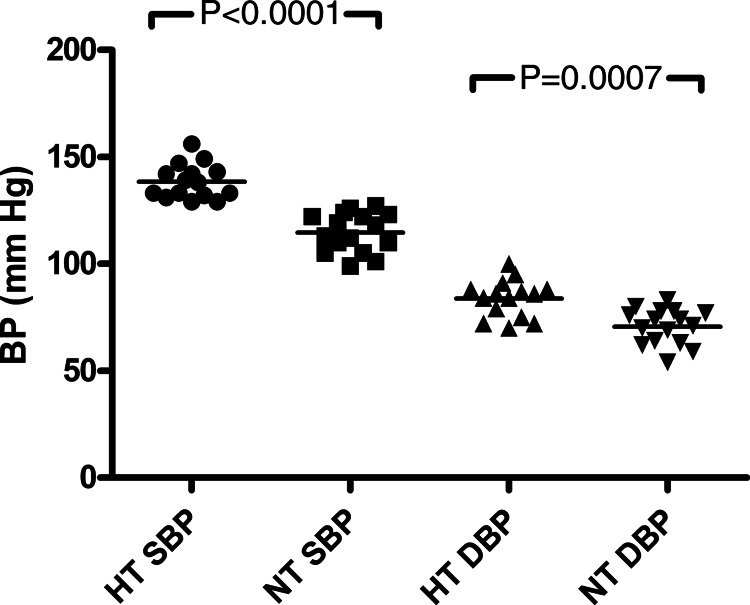
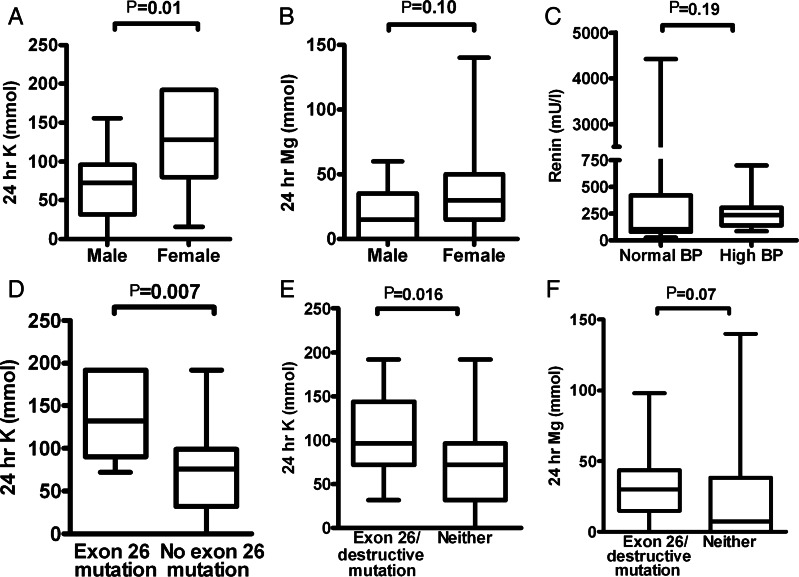
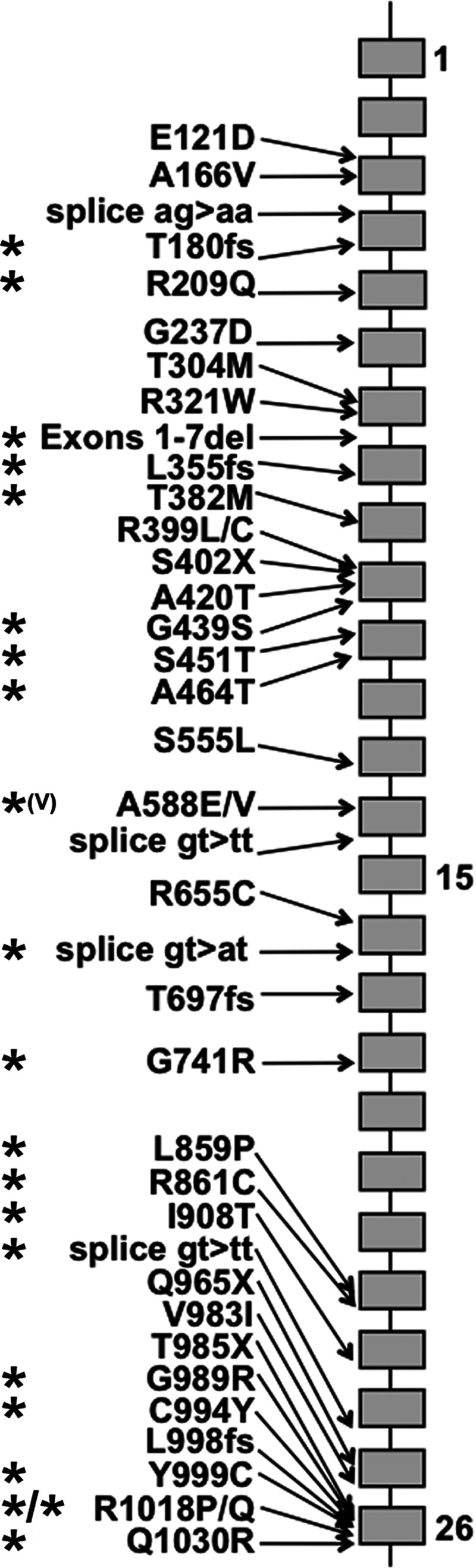
Results: The 21 males and 15 females were of median age 39.5 years, range 17-66 years. Six were diagnosed in childhood. Among the 72 mutant alleles, 41 different sequence alterations were identified, of which 13 were previously unreported. Surprisingly, 44% (n = 16) of the cohort has developed hypertension (13 males, 3 females, P = 0.019; median age 53 versus 57 years, P = 0.95). One was already hypertensive by age 23 years. Currently normotensive patients were significantly younger: median 37 versus 55 years (P = 0.005). Hypertensive patients were more likely to harbour mutations in the C-terminal half of the NCCT protein (P = 0.016). Females required more K (median 128 versus 72 mmol/day; P = 0.01) but not Mg. Those with exon 26 and/or at least one destructive mutation had higher K requirements than those with neither: 108 versus 72 mmol (P = 0.016) and a tendency towards higher Mg needs: 30 versus 7.4 mmol (P = 0.07).
Conclusions: Our findings suggest that the development of secondary hypertension may be an expected feature of the ageing GS population despite the obligate salt wasting that characterizes the disorder. We hypothesize that this may be related to chronic secondary hyperaldosteronism. The apparently more severe phenotype in women may be related to the effects of female sex hormones on expression or function of NCCT.
Keywords: Gitelman syndrome; distal convoluted tubule; hypertension; hypokalaemia; hypomagnesaemia.
Figures
Similar articles
-
Identification of compound mutations of SLC12A3 gene in a Chinese pedigree with Gitelman syndrome exhibiting Bartter syndrome-liked phenotypes.BMC Nephrol. 2020 Aug 5;21(1):328. doi: 10.1186/s12882-020-01996-2. BMC Nephrol. 2020. PMID: 32758178 Free PMC article.
-
Gitelman syndrome in a South African family presenting with hypokalaemia and unusual food cravings.BMC Nephrol. 2017 Jan 26;18(1):38. doi: 10.1186/s12882-017-0455-3. BMC Nephrol. 2017. PMID: 28125972 Free PMC article.
-
Phenotype-genotype correlation and follow-up in adult patients with hypokalaemia of renal origin suggesting Gitelman syndrome.Eur J Endocrinol. 2011 Oct;165(4):665-73. doi: 10.1530/EJE-11-0224. Epub 2011 Jul 13. Eur J Endocrinol. 2011. PMID: 21753071
-
A novel SLC12A3 homozygous c2039delG mutation in Gitelman syndrome with hypocalcemia.BMC Nephrol. 2018 Dec 17;19(1):362. doi: 10.1186/s12882-018-1163-3. BMC Nephrol. 2018. PMID: 30558554 Free PMC article. Review.
-
The genetic spectrum of Gitelman(-like) syndromes.Curr Opin Nephrol Hypertens. 2022 Sep 1;31(5):508-515. doi: 10.1097/MNH.0000000000000818. Epub 2022 Jul 11. Curr Opin Nephrol Hypertens. 2022. PMID: 35894287 Free PMC article. Review.
Cited by
-
Hypokalemic paralysis due to thyrotoxicosis accompanied by Gitelman's syndrome.Indian J Nephrol. 2015 Mar-Apr;25(2):103-5. doi: 10.4103/0971-4065.140719. Indian J Nephrol. 2015. PMID: 25838649 Free PMC article.
-
Gitelman Syndrome and Hypertension: A Case Report.Cureus. 2023 Sep 2;15(9):e44590. doi: 10.7759/cureus.44590. eCollection 2023 Sep. Cureus. 2023. PMID: 37795074 Free PMC article.
-
Acquired Gitelman Syndrome in an Anti-SSA Antibody-positive Patient with a SLC12A3 Heterozygous Mutation.Intern Med. 2016;55(21):3201-3204. doi: 10.2169/internalmedicine.55.6390. Epub 2016 Nov 1. Intern Med. 2016. PMID: 27803420 Free PMC article.
-
Clinicopathological Features of Gitelman Syndrome with Proteinuria and Renal Dysfunction.Nephron. 2023;147(9):531-540. doi: 10.1159/000529775. Epub 2023 Feb 20. Nephron. 2023. PMID: 36806220 Free PMC article.
-
Gitelman syndrome: an analysis of the underlying pathophysiologic mechanisms of acid-base and electrolyte abnormalities.Int Urol Nephrol. 2018 Jan;50(1):91-96. doi: 10.1007/s11255-017-1653-4. Epub 2017 Jul 25. Int Urol Nephrol. 2018. PMID: 28744758 Review.
References
-
- Gitelman HJ, Graham JB, Welt LG. A new familial disorder characterized by hypokalemia and hypomagnesemia. Trans Assoc Am Physicians. 1966;79:221–235. - PubMed
-
- Simon DB, Nelson-Williams C, Bia MJ, et al. Gitelman's variant of Bartter's syndrome, inherited hypokalaemic alkalosis, is caused by mutations in the thiazide-sensitive Na–Cl cotransporter. Nat Genet. 1996;12:24–30. - PubMed
-
- Lin SH, Cheng NL, Hsu YJ, et al. Intrafamilial phenotype variability in patients with Gitelman syndrome having the same mutations in their thiazide-sensitive sodium/chloride cotransporter. Am J Kidney Dis. 2004;43:304–312. - PubMed
-
- Riveira-Munoz E, Chang Q, Bindels RJ, et al. Gitelman's syndrome: towards genotype–phenotype correlations? Pediatr Nephrol. 2007;22:326–332. - PubMed
-
- Simon DB, Bindra RS, Mansfield TA, et al. Mutations in the chloride channel gene, CLCNKB, cause Bartter's syndrome type III. Nat Genet. 1997;17:171–178. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
