

Detection of anti-tat antibodies in CSF of individuals with HIV-associated neurocognitive disorders
- PMID: 23329164
- PMCID: PMC3593725
- DOI: 10.1007/s13365-012-0144-8
Detection of anti-tat antibodies in CSF of individuals with HIV-associated neurocognitive disorders
Abstract
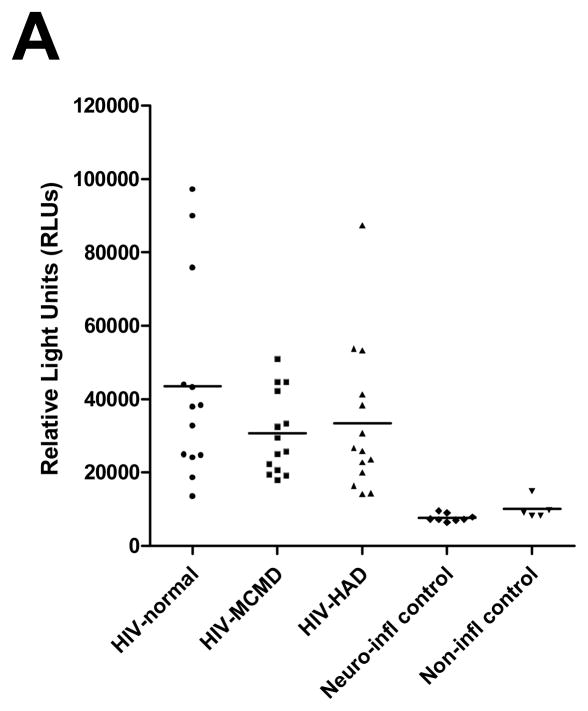
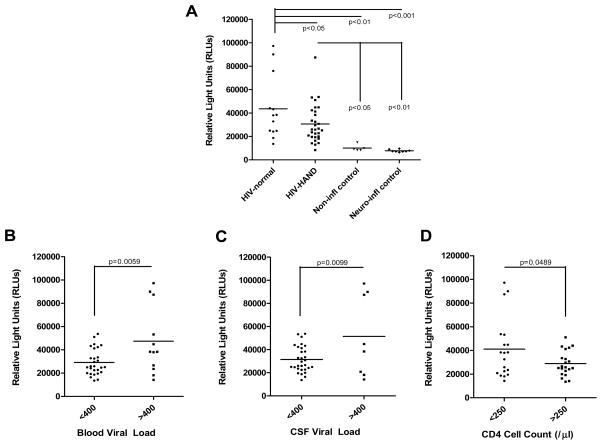
Despite major advances in the development of antiretroviral therapies, currently available treatments have no effect on the production of HIV-Tat protein once the proviral DNA is formed. Tat is a highly neurotoxic and neuroinflammatory protein, but its effects may be modulated by antibody responses against it. We developed an indirect enzyme-linked immunosorbent assay and measured anti-Tat antibody titers in CSF of a well characterized cohort of 52 HIV-infected and 13 control individuals. We successfully measured anti-Tat antibodies in CSF of HIV-infected individuals with excellent sensitivity and specificity, spanning a broad range of detection from 10,000 to over 100,000 relative light units. We analyzed them for relationship to cognitive function, CD4 cell counts, and HIV viral load. Anti-Tat antibody levels were higher in those without neurocognitive dysfunction than in those with HIV-associated neurocognitive dysfunction (HAND) and in individuals with lower CD4 cell counts and higher viral loads. We provide details of an assay which may have diagnostic, prognostic, or therapeutic implications for patients with HAND. Active viral replication may be needed to drive the immune response against Tat protein, but this robust immune response against the protein may be neuroprotective.
Figures
References
-
- Davis LE, Hjelle BL, Miller VE, Palmer DL, Llewellyn AL, Merlin TL, Young SA, Mills RG, Wachsman W, Wiley CA. Early viral brain invasion in iatrogenic human immunodeficiency virus infection. Neurology. 1992;42:1736–1739. - PubMed
-
- Dore GJ, McDonald A, Li Y, Kaldor JM, Brew BJ National HIVSC . Marked improvement in survival following AIDS dementia complex in the era of highly active antiretroviral therapy. AIDS (London, England) 2003;17:1539–1545. - PubMed
-
- Gonzalez E, Rovin BH, Sen L, Cooke G, Dhanda R, Mummidi S, Kulkarni H, Bamshad MJ, Telles V, Anderson SA, Walter EA, Stephan KT, Deucher M, Mangano A, Bologna R, Ahuja SS, Dolan MJ, Ahuja SK. HIV-1 infection and AIDS dementia are influenced by a mutant MCP-1 allele linked to increased monocyte infiltration of tissues and MCP-1 levels. Proceedings of the National Academy of Sciences of the United States of America. 2002;99:13795–13800. - PMC - PubMed
-
- Haughey NJ, Nath A, Mattson MP, Slevin JT, Geiger JD. HIV-1 Tat through phosphorylation of NMDA receptors potentiates glutamate excitotoxicity. Journal of neurochemistry. 2001;78:457–467. - PubMed
-
- Hudson L, Liu J, Nath A, Jones M, Raghavan R, Narayan O, Male D, Everall I. Detection of the human immunodeficiency virus regulatory protein tat in CNS tissues. Journal of neurovirology. 2000;6:145–155. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
