

Prognostic value of Ki-67 for prostate cancer death in a conservatively managed cohort
- PMID: 23329234
- PMCID: PMC3566811
- DOI: 10.1038/bjc.2012.598
Prognostic value of Ki-67 for prostate cancer death in a conservatively managed cohort
Abstract
Background: Standard clinical parameters cannot accurately differentiate indolent from aggressive prostate cancer. Our previous work showed that immunohistochemical (IHC) Ki-67 improved prediction of prostate cancer death in a cohort of conservatively treated clinically localised prostate cancers diagnosed by transurethral resection of the prostate (TURP). Here, we present results in a more clinically relevant needle biopsy cohort.
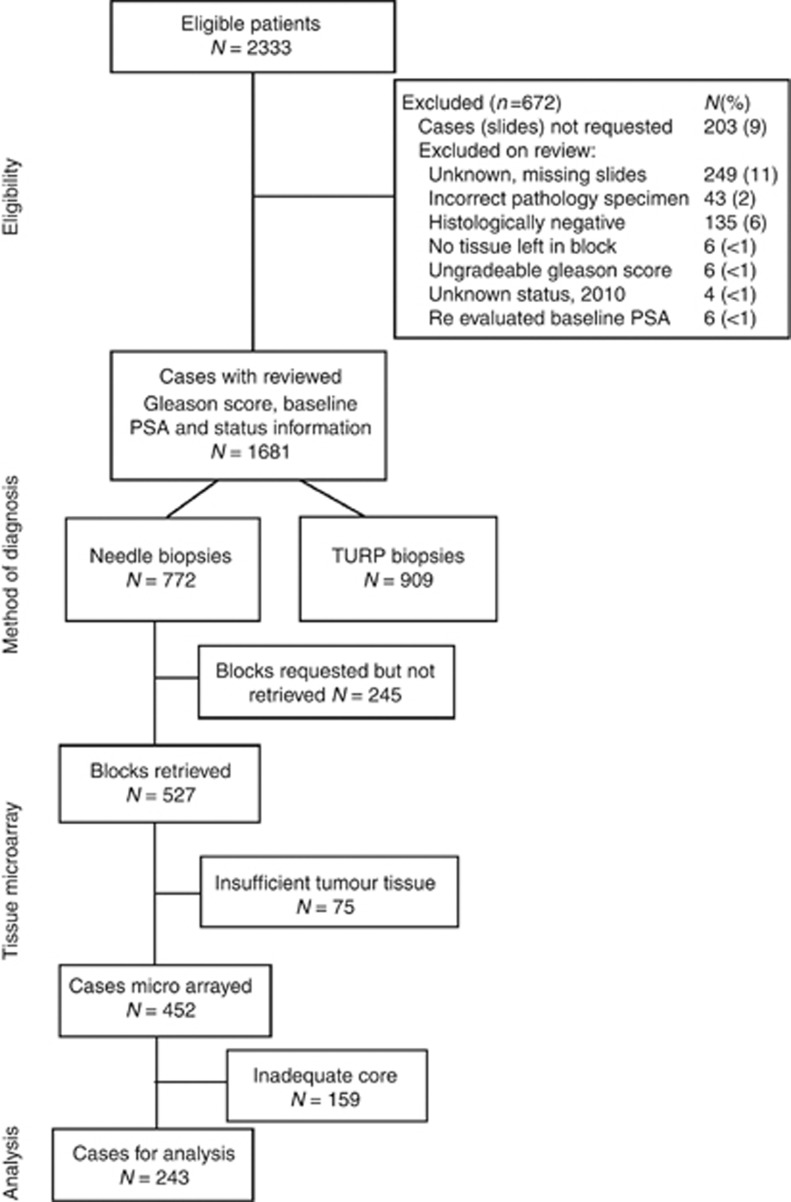
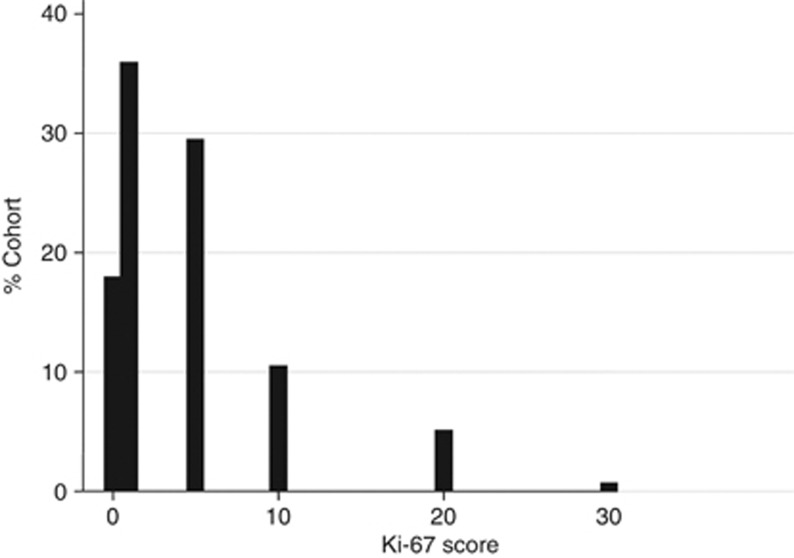
Methods: Biopsy specimens were microarrayed. The percentage of Ki-67 positively stained malignant cells per core was measured and the maximum score per individual used in analysis of time to death from prostate cancer using a Cox proportional hazards model.
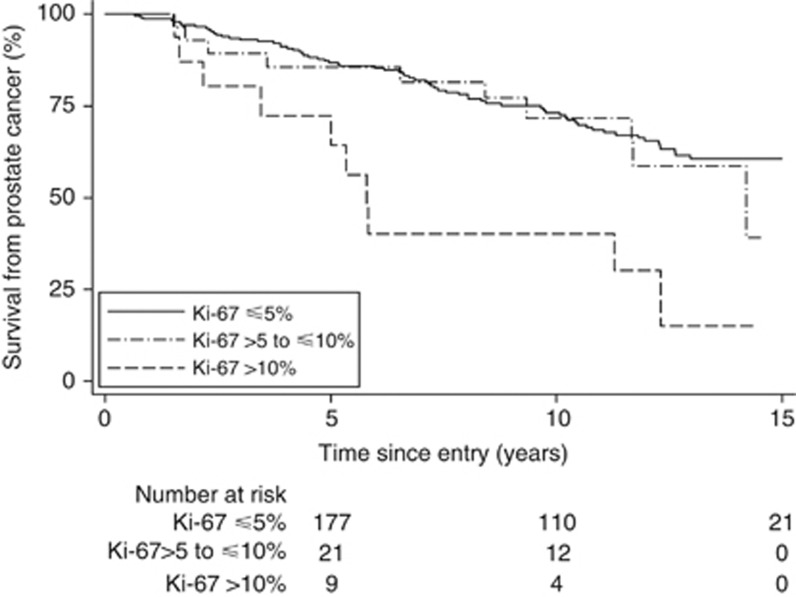
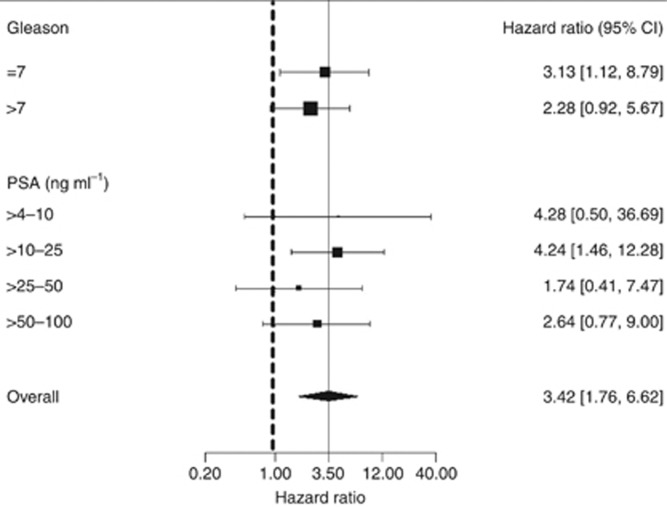
Results: In univariate analysis (n=293), the hazard ratio (HR) (95% confidence intervals) for dichotomous Ki-67 (≤ 10%, >10%) was 3.42 (1.76, 6.62) χ(2) (1 df)=9.8, P=0.002. In multivariate analysis, Ki-67 added significant predictive information to that provided by Gleason score and prostate-specific antigen (HR=2.78 (1.42, 5.46), χ(2) (1 df)=7.0, P=0.008).
Conclusion: The IHC Ki-67 scoring on prostate needle biopsies is practicable and yielded significant prognostic information. It was less informative than in the previous TURP cohort where tumour samples were larger and more comprehensive, but in more contemporary cohorts with larger numbers of biopsies per patient, Ki-67 may prove a more powerful biomarker.
Figures
References
-
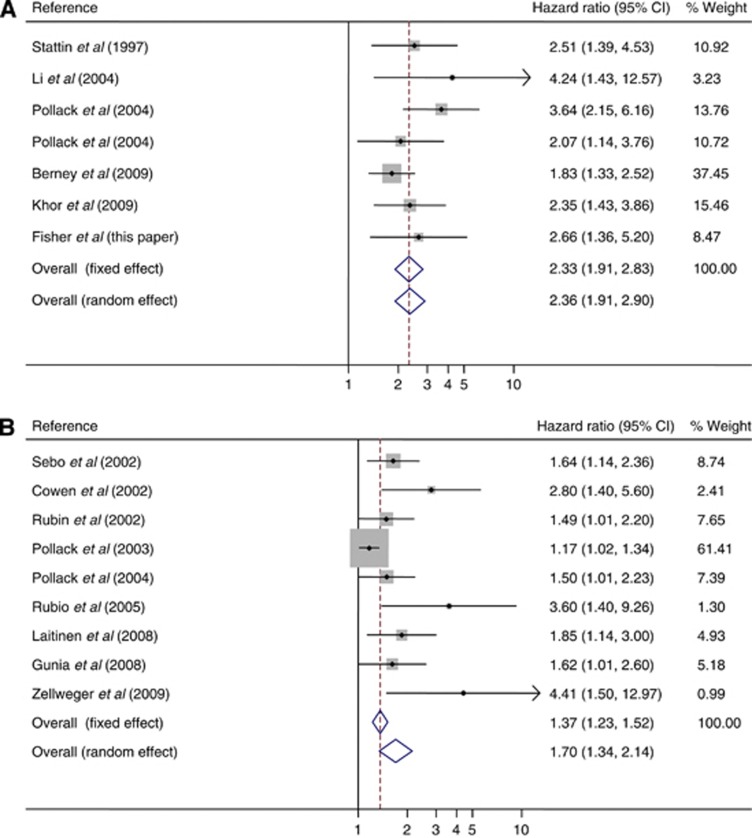
- Berney DM, Gopalan A, Kudahetti S, Fisher G, Ambroisine L, Foster CS, Reuter V, Eastham J, Moller H, Kattan MW, Gerald W, Cooper C, Scardino P, Cuzick J. Ki-67 and outcome in clinically localised prostate cancer: analysis of conservatively treated prostate cancer patients from the Trans-Atlantic Prostate Group study. Br J Cancer. 2009;100 (6:888–893. - PMC - PubMed
-
- Cowen D, Troncoso P, Khoo VS, Zagars GK, von Eschenbach AC, Meistrich ML, Pollack A. Ki-67 staining is an independent correlate of biochemical failure in prostate cancer treated with radiotherapy. Clin Cancer Res. 2002;8 (5:1148–1154. - PubMed
-
- Cuzick J, Berney DM, Fisher G, Mesher D, Møller H, Reid JE, Perry M, Park J, Younus A, Gutin A, Foster CS, Scardino P, Lanchbury JS, Stone S, on behalf of the Transatlantic Prostate Group Prognostic value of a cell cycle progression signature for prostate cancer death in a conservatively managed needle biopsy cohort. Br J Cancer. 2012;106:1095–1099. - PMC - PubMed
-
- Cuzick J, Swanson GP, Fisher G, Brothman AR, Berney DM, Reid JE, Mesher D, Speights VO, Stankiewicz E, Foster CS, Møller H, Scardino P, Warren JD, Park J, Younus A, Flake DD, Wagner S, Gutin A, Lanchbury JS, Stone S, Transatlantic Prostate Group Prognostic value of an RNA expression signature derived from cell cycle proliferation genes in patients with prostate cancer: a retrospective study. Lancet Oncol. 2011;12 (3:245–255. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
