

Review
doi: 10.1590/s1678-77572012000600013.
Partial maxillary osteotomy following an unsuccessful forced eruption of an impacted maxillary canine: 10 year follow-up. Review and case report
Affiliations
- PMID: 23329250
- PMCID: PMC3881860
- DOI: 10.1590/s1678-77572012000600013
Item in Clipboard
Review
Partial maxillary osteotomy following an unsuccessful forced eruption of an impacted maxillary canine: 10 year follow-up. Review and case report
J Appl Oral Sci.
2012 Nov-Dec.
Abstract
The maxillary canines are amongst the most frequently impacted teeth, second only to the third molars. Several conservative orthodontic and surgical techniques are available to position the teeth properly in the dental arch, even in severe cases. However, when an extraction is necessary, it often leaves a critical alveolar defect of difficult management. The authors present the technique of partial maxillary osteotomy, in which a dento-alveolar segment is moved mesially, hence closing the remaining space, allowing for the formation of healthy periodontium and resulting in an adequate functional and aesthetic outcome. A case report is presented with a 10 year follow-up, proving the technique's stability in the long term.
Figures
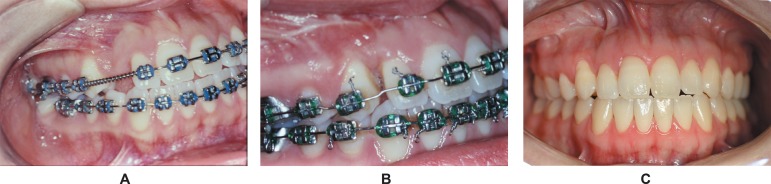
A. Preoperatory aspect. Orthodontic appliance was used to open space for the right
maxillary canine traction. B. Oclusion in 30 days postoperative control. Tooth 14
substitutes the lost canine, with closure of the space, in the horizontal
immobilization stage, prior to orthodontic alignment. C. Clinical control of 10
years and 10 months postoperatively. Orthodontic appliances were removed for 10
years and 3 months. Patient's occlusion maintains excellent functional and
esthetic result
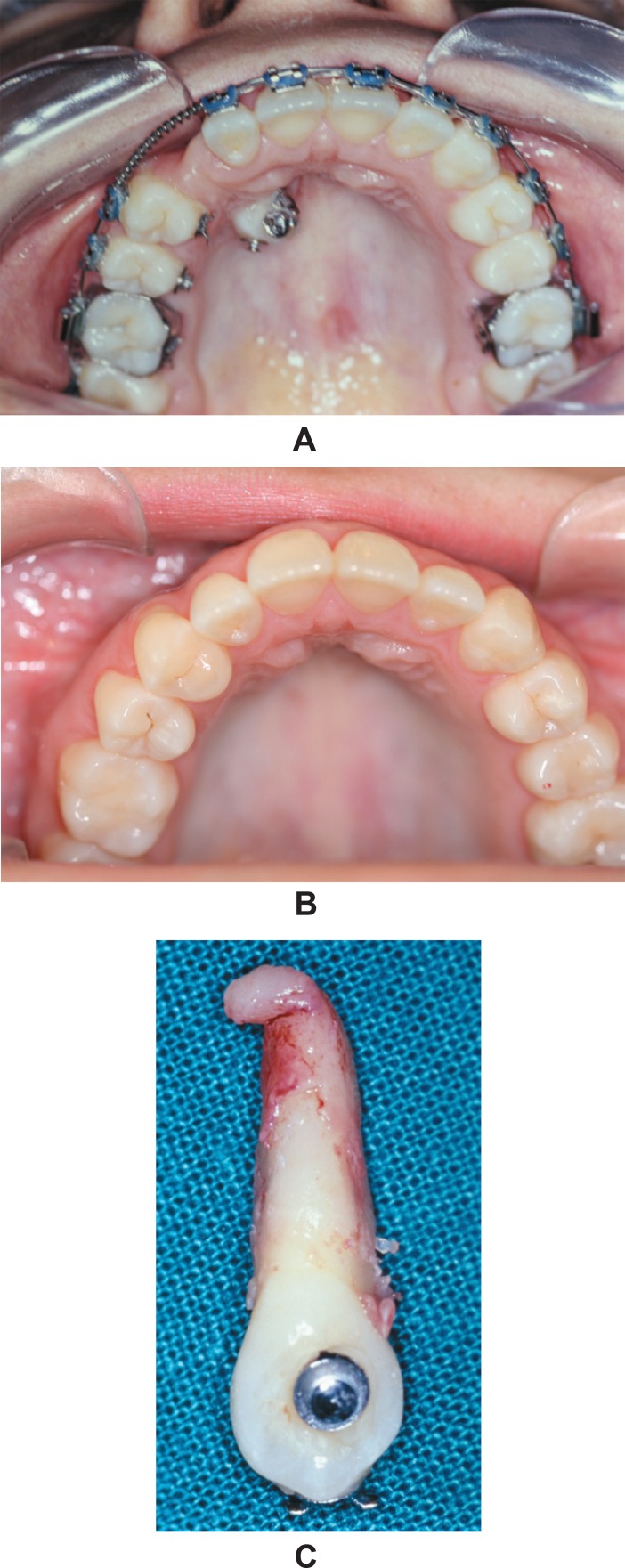
Palatal view. A. Preoperatory. Tooth 13 partially erupted in a transalveolar
position with the crown mesially inclined. Note the presence of three orthodontic
traction devices. B. Clinical control of 10 years and 10 months postoperatively,
with orthodontic appliance removed for 10 years and 3 months, thus confirming
stability. Vestibular and palatal gingival contour is maintained. C. Extracted
maxillary right canine. Severe apical dilaceration is observed, along with areas
compatible with periodontal alterations, possibly related to root ankylosis
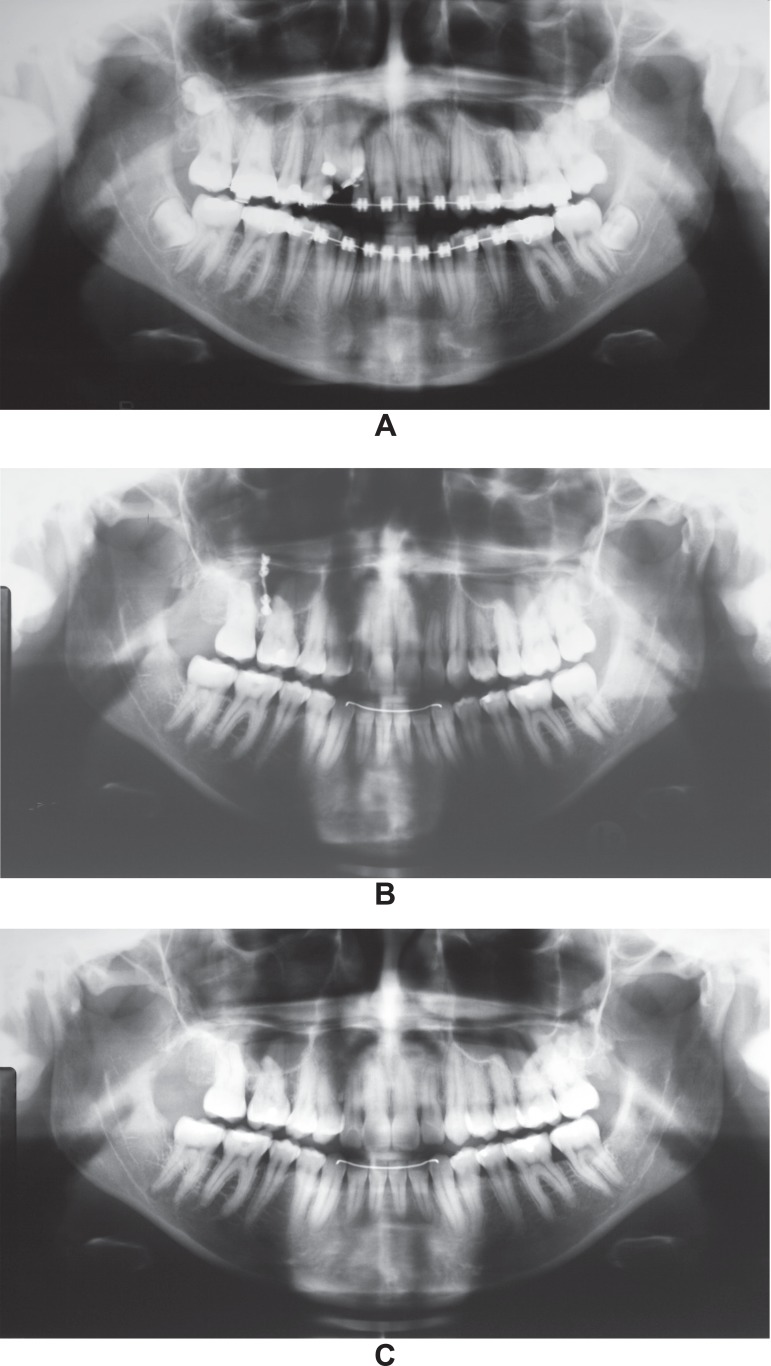
Panoramic radiographic sequence. A. Preoperative aspect dating from January 14,
2001. Alveolar bone loss is noticeable along the misaligned impacted canine’s
crown. B. Control of October, 2010. The osteosynthesis titanium miniplate is still
present. Alveolar bone neoformation and remodeling are completed with the
mobilization and approximation of the posterior segment. C. Following removal of
the fixation, panoramic radiographic control of January, 17, 2012
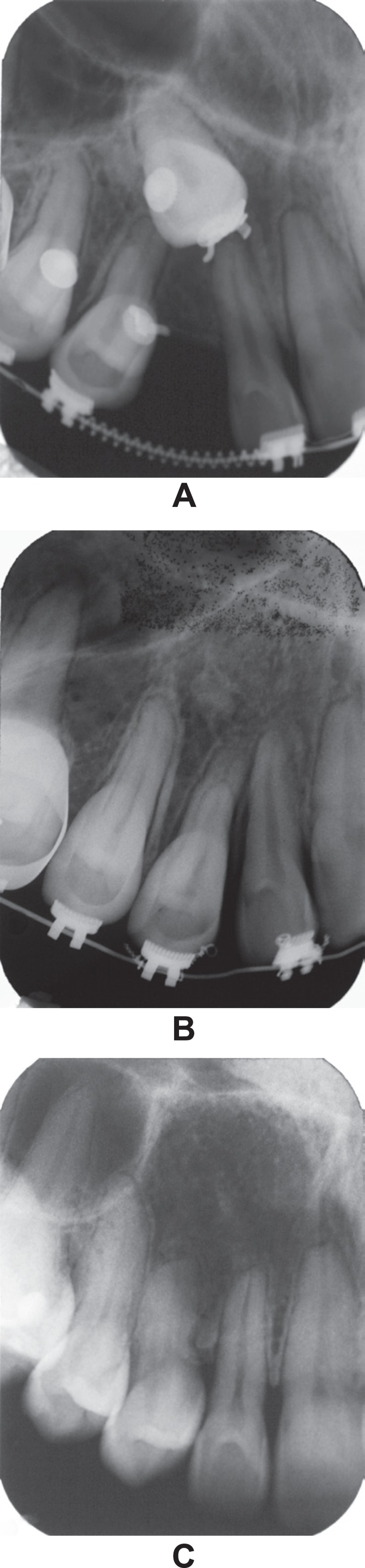
Periapical radiographic sequence. A. Preoperatory image of January 14, 2001. The
root apex is perfectly identifiable situated between the nasal and sinusal
cortical, area named the Ennis inverted Y. In this image, root dilaceration is not
noticeable. B. Periapical radiography of September 10, 2001, corresponding to 4
months and 7 days following surgery. Alveolar bone height may be observed between
teeth 12 and 14 with the distal dental-alveolar segment approximation. C.
Periapical radiography of January 17, 2001, corresponding to 10 years and 10
months following surgery. Space closure and complete bone neoformation and
remodeling are apparent, typifying normal physiology of the area. All involved
teeth maintain pulpar vitality
Similar articles
-
Maxillary canine impactions related to impacted central incisors: two case reports.J Contemp Dent Pract. 2007 Sep 1;8(6):72-81. J Contemp Dent Pract. 2007. PMID: 17846674
-
Open surgical approach to a maxillary impacted canine: a case report.Int J Orthod Milwaukee. 2013 Fall;24(3):25-8. Int J Orthod Milwaukee. 2013. PMID: 24358653
-
Efficacy of the technique of piezoelectric corticotomy for orthodontic traction of impacted mandibular third molars.Br J Oral Maxillofac Surg. 2015 Apr;53(4):326-31. doi: 10.1016/j.bjoms.2015.01.002. Epub 2015 Jan 28. Br J Oral Maxillofac Surg. 2015. PMID: 25638568 Clinical Trial.
-
Forced eruption of a labially impacted maxillary canine with a transcoronal stainless wire: report of case.ASDC J Dent Child. 2000 Jul-Aug;67(4):288-92. ASDC J Dent Child. 2000. PMID: 10997247 Review.
-
Office-based procedures for unusual impactions.Atlas Oral Maxillofac Surg Clin North Am. 2013 Sep;21(2):211-20. doi: 10.1016/j.cxom.2013.06.001. Atlas Oral Maxillofac Surg Clin North Am. 2013. PMID: 23981496 Review. No abstract available.
References
-
- Alessandri Bonetti G, Incerti Parenti S, Daprile G, Montevecchi M. Failure after closed traction of an unerupted maxillary permanent canine: diagnosis and treatment planning. Am J Orthod Dentofacial Orthop. 2011;140:121–125. - PubMed
-
- Alqerban A, Jacobs R, Fieuws S, Nackaerts O, SEDENTEXCT Project Consortium, Willems G. Comparison of 6 cone-beam computed tomography systems for image quality and detection of simulated canine impaction-induced external root resorption in maxillary lateral incisors. Am J Orthod Dentofacial Orthop. 2011;140:129–139. - PubMed
-
- Bass TB. Observations on the misplaced upper canine tooth. Dental Pract Dent Rec. 1967;18:25–33. - PubMed
-
- Becker A, Chaushu G, Chaushu S. Analysis of failure in the treatment of impacted maxillary canines. Am J Orthod Dentofacial Orthop. 2010;137:743–754. - PubMed
-
- Bishara SE. Impacted maxillary canines: a review. Am J Orthod Dentofacial Orthop. 1992;101:159–171. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
