

Driving with central field loss I: effect of central scotomas on responses to hazards
- PMID: 23329309
- PMCID: PMC3605225
- DOI: 10.1001/jamaophthalmol.2013.1443
Driving with central field loss I: effect of central scotomas on responses to hazards
Abstract
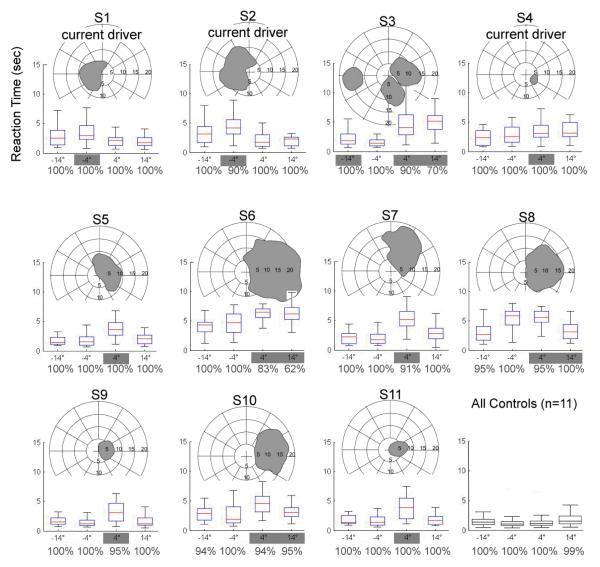
Objectives: To determine how central field loss (CFL) affects reaction time to pedestrians and to test the hypothesis that scotomas lateral to the preferred retinal locus will delay detection of hazards approaching from that side.
Methods: Participants with binocular CFL (scotoma diameter, 7°-25°; visual acuity, 0.3-1.0 logMAR) using lateral preferred retinal fixation loci and matched controls with normal vision drove in a simulator for approximately 1½ hours per session for 2 sessions a week apart. Participants responded to frequent virtual pedestrians who appeared on either the left or right sides and approached the participant's lane on a collision trajectory that, therefore, caused them to remain in approximately the same area of the visual field.
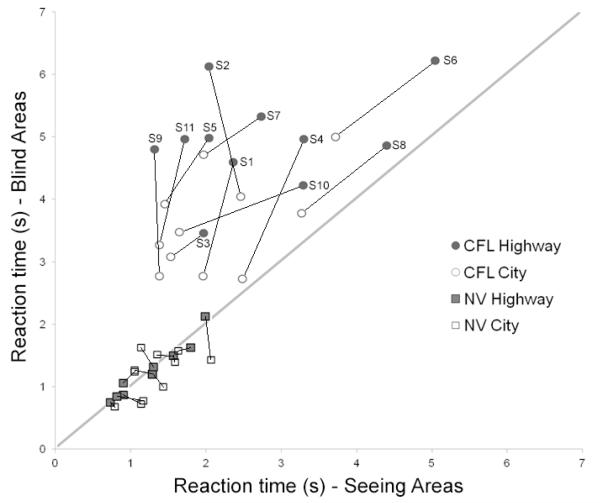
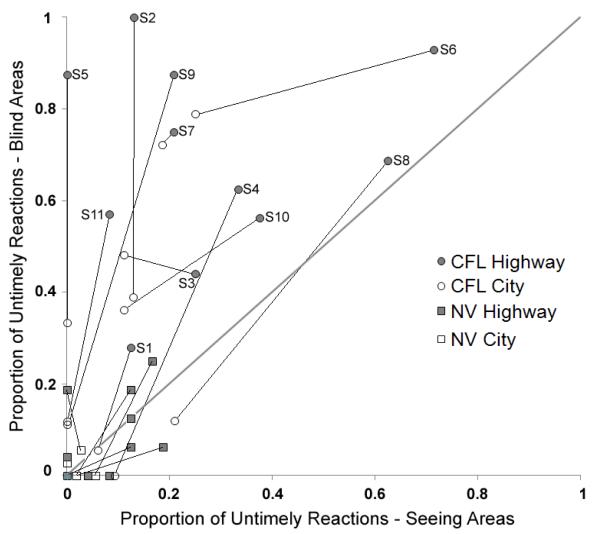
Results: The study included 11 individuals with CFL and 11 controls with normal vision. The CFL participants had more detection failures for pedestrians who appeared in areas of visual field loss than did controls in corresponding areas (6.4% vs 0.2%). Furthermore, the CFL participants reacted more slowly to pedestrians in blind than nonscotomatous areas (4.28 vs 2.43 seconds, P < .001) and overall had more late and missed responses than controls (29% vs 3%, P < .001). Scotoma size and contrast sensitivity predicted outcomes in blind and seeing areas, respectively. Visual acuity was not correlated with response measures.
Conclusions: In addition to causing visual acuity and contrast sensitivity loss, the central scotoma per se delayed hazard detection even though small eye movements could potentially compensate for the loss. Responses in nonscotomatous areas were also delayed, although to a lesser extent, possibly because of the eccentricity of fixation. Our findings will help practitioners advise patients with CFL about specific difficulties they may face when driving.
Figures
Comment in
-
Driving with central field loss.JAMA Ophthalmol. 2013 Mar;131(3):393-5. doi: 10.1001/jamaophthalmol.2013.1974. JAMA Ophthalmol. 2013. PMID: 23329348 No abstract available.
-
Central visual field loss and driving.JAMA Ophthalmol. 2013 Jun;131(6):819-21. doi: 10.1001/jamaophthalmol.2013.434. JAMA Ophthalmol. 2013. PMID: 23764711 No abstract available.
-
Central visual field loss and driving--reply.JAMA Ophthalmol. 2013 Jun;131(6):819-21. doi: 10.1001/jamaophthalmol.2013.4259. JAMA Ophthalmol. 2013. PMID: 23764712 Free PMC article. No abstract available.
References
-
- Petzold A, Plant GT. Central and paracentral visual field defects and driving abilities. Ophthalmologica. 2005;219:191–201. - PubMed
-
- Timberlake GT, Peli E, Essock EA, Augliere RA. Reading with macular scomata II: Retinal locus for scanning text. Invest. Ophthalmol. Vis. Sci. 1987;28:1268–121274. - PubMed
-
- Verezen CA, Hoyng CB, Meulendijks CF, Keunen JE, Klevering BJ. Eccentric gaze direction in patients with central field loss. Optom. Vis. Sci. 2011;88:1164–1171. - PubMed
-
- Fletcher DC, Schuchard RA. Preferred retinal loci relationship to macular scotomas in a low-vision population. Ophthalmology. 1997;104:632–638. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
