

Where is the culprit? A case of acromegaly that defied the management algorithm
- PMID: 23329711
- PMCID: PMC3604022
- DOI: 10.1136/bcr-2012-007604
Where is the culprit? A case of acromegaly that defied the management algorithm
Abstract
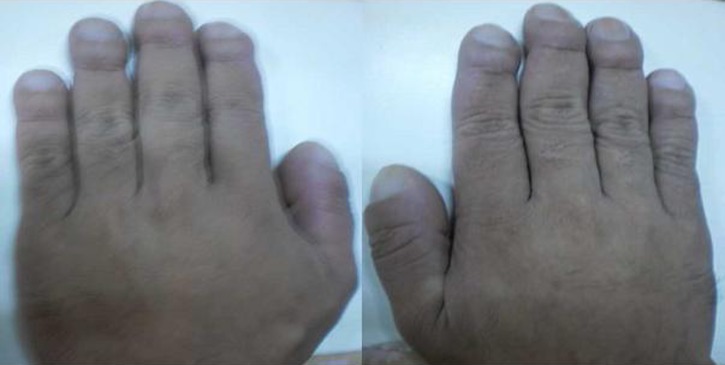
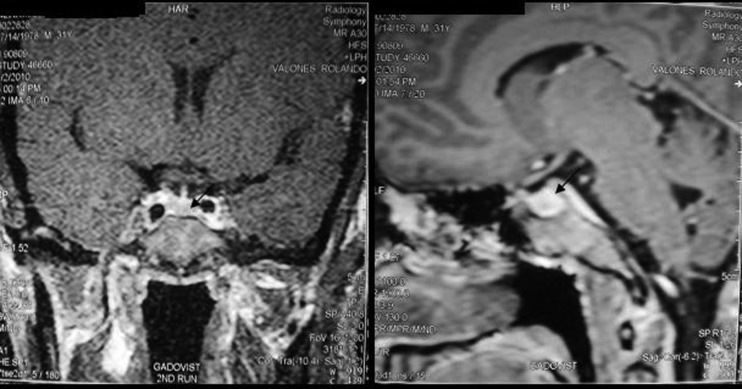
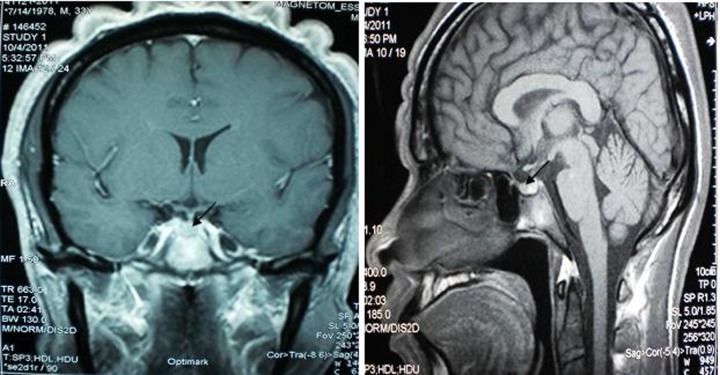
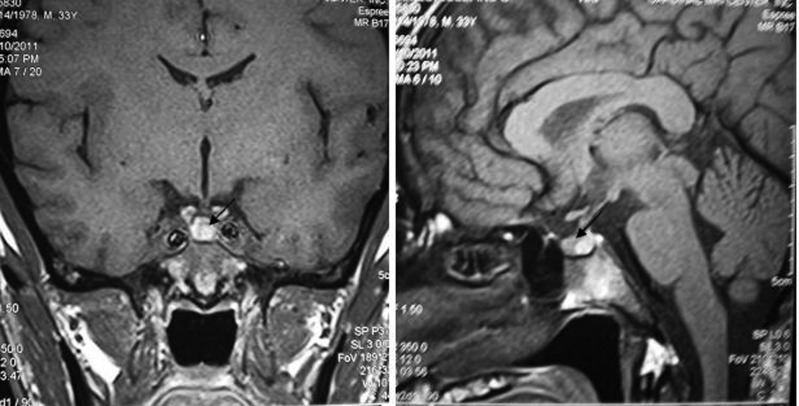
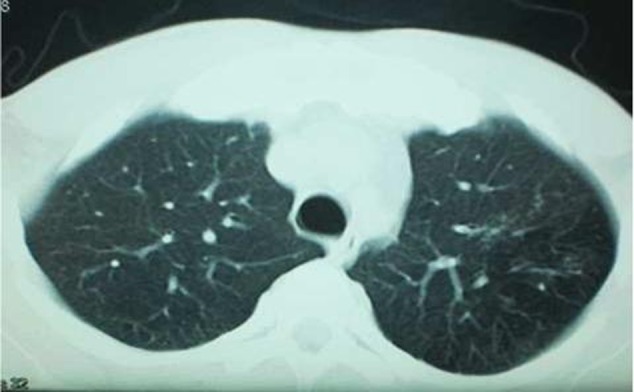
A 30-year-old Filipino man presented with a 11-year history of coarse facial features and progressive enlargement of hands and feet. Initial work-up revealed elevated insulin-like growth factor-1 and non-suppressible growth hormone level after 75 g glucose challenge test. Initial cranial MRI performed in the year 2010 showed absence of pituitary adenoma. The patient was lost to follow-up. He again consulted in the year 2011 and a repeat cranial MRI and a dedicated pituitary MRI were performed and both did not reveal any pituitary mass. Further investigation included chest and abdominal CT scan, both of which did not show any neoplasm. At present, there has been no practice guideline on the management of acromegalic patients on whom the identifiable source cannot be found. The patient was given the option to undergo surgical exploration of the pituitary gland or medical treatment with somatostatin analogues. He decided to undergo surgery but has not given consent for the procedure.
Figures



Similar articles
-
Acromegaly.Pituitary. 2006;9(4):297-303. doi: 10.1007/s11102-006-0409-4. Pituitary. 2006. PMID: 17077948 Review.
-
Potential antitumour activity of pasireotide on pituitary tumours in acromegaly.Lancet Diabetes Endocrinol. 2019 Jun;7(6):425-426. doi: 10.1016/S2213-8587(19)30113-5. Epub 2019 Apr 4. Lancet Diabetes Endocrinol. 2019. PMID: 30956093 No abstract available.
-
Current pharmacotherapy for acromegaly: a review.Expert Opin Pharmacother. 2005 Nov;6(14):2393-405. doi: 10.1517/14656566.6.14.2393. Expert Opin Pharmacother. 2005. PMID: 16259571 Review.
-
Neuroendocrine tumors secreting growth hormone-releasing hormone: Pathophysiological and clinical aspects.Pituitary. 2006;9(3):221-9. doi: 10.1007/s11102-006-0267-0. Pituitary. 2006. PMID: 17036195 Review.
-
Dissociation between tumor shrinkage and hormonal response during somatostatin analog treatment in an acromegalic patient: preferential expression of somatostatin receptor subtype 3.J Endocrinol Invest. 2006 Oct;29(9):826-30. doi: 10.1007/BF03347378. J Endocrinol Invest. 2006. PMID: 17114915
References
-
- Cook D, Ezzat S, Katznelson L, et al. American association of clinical endocrinologists medical guidelines for clinical practice for the diagnosis and treatment of acromegaly. Endocr Pract 2004;10:213–25 - PubMed
-
- Teh BT, Kytola S, Farnebo F, et al. Mutation analysis of the MEN 1 gene in multiple endocrine neoplasia type 1, familial acromegaly and familial isolated hyperparathyroidism. J Clin Endocrinol Metab 1998;83:2621–6 - PubMed
-
- Benlian P, Giraud S, Lahlou N, et al. Familial acromegaly: a specific clinical entity: further evidence from the genetic study of a three-generation family. Eur J Endocrinol 1995;133:451–6 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources