

Radiofrequency catheter ablation of idiopathic right ventricular outflow tract arrhythmias
- PMID: 23329871
- PMCID: PMC3540113
- DOI: 10.1016/s0972-6292(16)30585-x
Radiofrequency catheter ablation of idiopathic right ventricular outflow tract arrhythmias
Abstract
Idiopathic ventricular arrhythmias (VA) consist of various subtypes of VA that occur in the absence of clinically apparent structural heart disease. Affected patients account for approximately 10% of all patients referred for evaluation of ventricular tachycardia (VT). Arrhythmias arising from the outflow tract (OT) are the most common subtype of idiopathic VA and more than 70-80% of idiopathic VTs or premature ventricular contractions (PVCs) originate from the right ventricular (RV) OT. Idiopathic OT arrhythmias are thought to be caused by adenosine-sensitive, cyclic adenosine monophosphate (cAMP) mediated triggered activity and, in general, manifest at a relatively early age. Usually they present as salvos of paroxysmal ventricular ectopic beats and are rarely life-threatening. When highly symptomatic and refractory to antiarrhythmic therapy or causative for ventricular dysfunction, ablation is a recommended treatment with a high success rate and a low risk of complications.
Keywords: ICDs; ablation; outflow tract; premature ventricular contractions; ventricular arrhythmias.
Figures
References
-
- Aliot EM, et al. EHRA/HRS Expert Consensus on Catheter Ablation of Ventricular Arrhythmias: developed in a partnership with the European Heart Rhythm Association (EHRA), a Registered Branch of the European Society of Cardiology (ESC), and the Heart Rhythm Society (HRS); in collaboration with the American College of Cardiology (ACC) and the American Heart Association (AHA) Europace . 2009;11:771. - PubMed
-
- Movsowitz C, et al. Idiopathic right ventricular outflow tract tachycardia: narrowing the anatomic location for successful ablation. Am Heart J. 1996;131:930. - PubMed
-
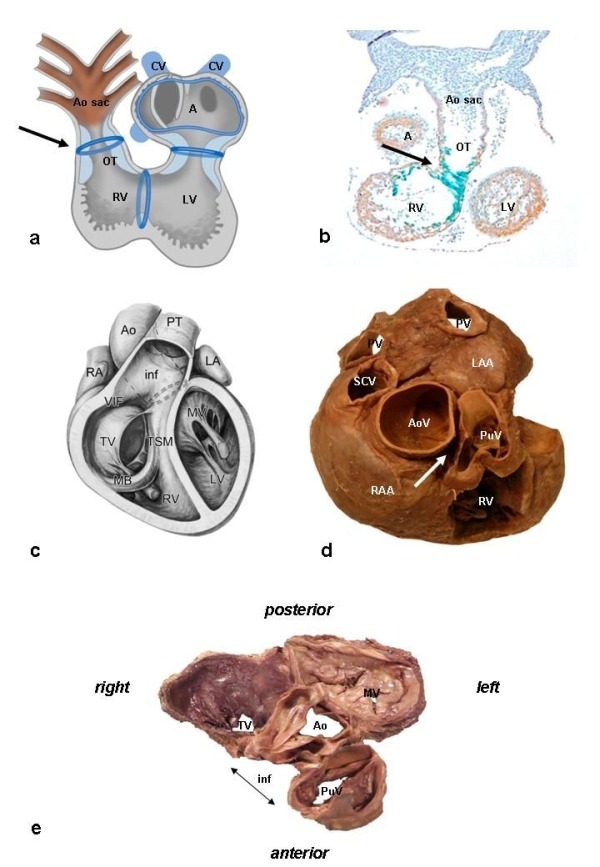
- Gittenberger-de Groot AC, et al. Basics of cardiac development for the understanding of congenital heart malformations. Pediatr Res. 2005;57:169. - PubMed
-
- Bartelings MM, et al. Morphogenetic considerations on congenital malformations of the outflow tract. Part 1: Common arterial trunk and tetralogy of Fallot. Int J Cardiol. 1991;32:213. - PubMed
LinkOut - more resources
Full Text Sources