

Fracture after androgen deprivation therapy among men with a high baseline risk of skeletal complications
- PMID: 23331464
- PMCID: PMC3625488
- DOI: 10.1111/j.1464-410X.2012.11758.x
Fracture after androgen deprivation therapy among men with a high baseline risk of skeletal complications
Abstract
WHAT'S KNOWN ON THE SUBJECT? AND WHAT DOES THE STUDY ADD?: Receipt of androgen deprivation therapy (ADT) has been associated with an increased risk of skeletal-associated complications, such as a decrease in bone mineral density and an increase in fracture risk. Many men with pre-existing health conditions receive ADT as their primary treatment because they are considered to be inappropriate candidates for attempted curative treatments. However, several chronic health conditions, such as diabetes, rheumatoid disease and chronic liver disease, are strong predictors for osteoporosis and fractures. We undertook the present study aiming to quantify the impact of treating men with ADT who carry known risk factors for skeletal complications. Among these high-risk men, more than 58% develop at least one fracture after ADT within the 12 years of follow-up. Men who sustained a fracture within 48 months experienced an almost 40% higher risk of mortality than those who did not. Our findings suggest that treating men with a high fracture risk at baseline with long-term ADT may have serious adverse consequences.
Objective: To quantify the impact of androgen deprivation therapy (ADT) in men with a high baseline risk of skeletal complications and evaluate the risk of mortality after a fracture.
Patients and methods: We studied 75994 men, aged ≥ 66 years, with localized prostate cancer from the Surveillance, Epidemiology and End Results-Medicare linked data. Cox proportional hazard models were employed to evaluate the risk.
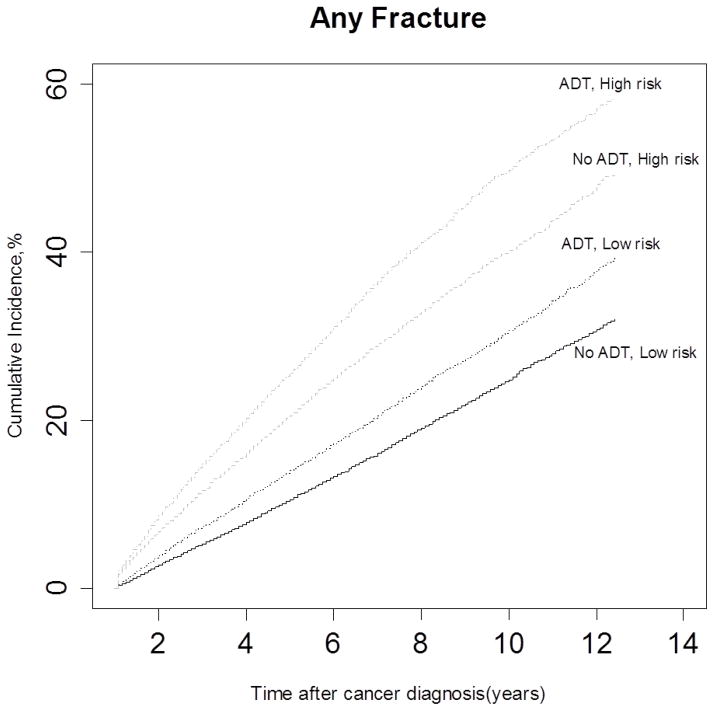
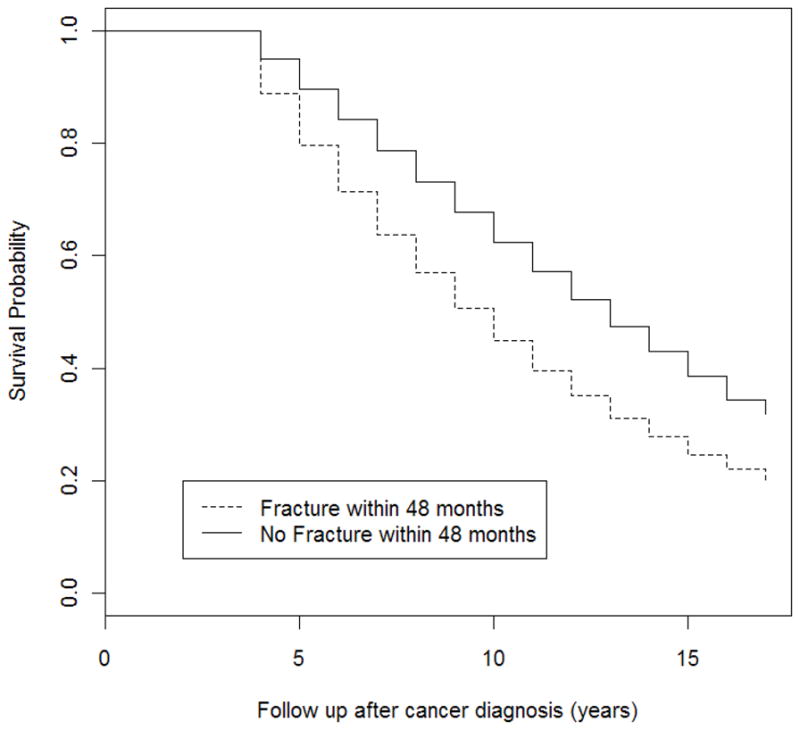
Results: Men with a high baseline risk of skeletal complications have a higher probability of receiving ADT than those with a low risk (52.1% vs 38.2%, P < 0.001). During the 12-year follow-up, more than 58% of men with a high risk and 38% of men with a low risk developed at least one fracture after ADT. The dose effect of ADT is stronger among men who received ADT only compared to those who received ADT with other treatments. In the high-risk group, the fracture rate increased by 19.9 per 1000 person-years (from 52.9 to 73.0 person-years) for men who did not receive ADT compared to those who received 18 or more doses of gonadotropin-releasing hormone agonist among men who received ADT only, and by 14.2 per 1000 person-years (from 45.2 to 59.4 person-years) among men who received ADT and other treatments. Men experiencing a fracture had a 1.38-fold higher overall mortality risk than those who did not (95% CI, 1.34-1.43).
Conclusions: Men with a high baseline risk of skeletal complications developed more fractures after ADT. The mortality risk is 40% higher after experiencing a fracture. Consideration of patient risk before prescribing ADT for long-term use may reduce both fracture risk and fracture-associated mortality.
© 2013 BJU International.
Conflict of interest statement
All authors declare that they have no conflicts of interest.
Figures
Comment in
-
Androgen deprivation therapy: further confirmation of known harms.BJU Int. 2013 May;111(5):690-1. doi: 10.1111/j.1464-410X.2013.11797.x. Epub 2013 Feb 18. BJU Int. 2013. PMID: 23418703 No abstract available.
-
Re: fracture after androgen deprivation therapy among men with a high baseline risk of skeletal complications.J Urol. 2014 Feb;191(2):388. doi: 10.1016/j.juro.2013.10.009. Epub 2013 Oct 3. J Urol. 2014. PMID: 24411874 No abstract available.
References
-
- Shahinian VB, Kuo Y-F, Gilbert SM. Reimbursement policy and androgen-deprivation therapy for prostate cancer. N Engl J Med. 2010;363:1822–32. - PubMed
-
- Shahinian VB, Kuo YF, Freeman JL, Goodwin JS. Risk of fracture after androgen deprivation for prostate cancer. N Engl J Med. 2005;352:154–64. - PubMed
-
- Smith MR, Boyce SP, Moyneur E, Duh MS, Raut MK, Brandman J. Risk of clinical fractures after gonadotropin-releasing hormone agonist therapy for prostate cancer. J Urol. 2006;175:136–9. - PubMed
-
- Smith MR, Lee WC, Brandman J, Wang Q, Botteman M, Pashos CL. Gonadotropin-releasing hormone agonists and fracture risk: a claims-based cohort study of men with nonmetastatic prostate cancer. J Clin Oncol. 2005;23:7897–903. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
