

Markers of inflammation and CD8 T-cell activation, but not monocyte activation, are associated with subclinical carotid artery disease in HIV-infected individuals
- PMID: 23332012
- PMCID: PMC3640592
- DOI: 10.1111/hiv.12013
Markers of inflammation and CD8 T-cell activation, but not monocyte activation, are associated with subclinical carotid artery disease in HIV-infected individuals
Abstract
Objectives: The aim of the study was to explore the relationships between lymphocyte and monocyte activation, inflammation, and subclinical vascular disease among HIV-1-infected patients on antiretroviral therapy (ART).
Methods: Baseline mean common carotid artery (CCA) intima-media thickness (IMT) and carotid plaque (IMT > 1.5 cm) were evaluated in the first 60 subjects enrolled in the Stopping Atherosclerosis and Treating Unhealthy Bone with Rosuvastatin in HIV (SATURN-HIV) trial. All subjects were adults on stable ART with evidence of heightened T-cell activation (CD8(+)CD38(+)HLA-DR(+) ≥ 19%) or increased inflammation (high-sensitivity C-reactive protein ≥ 2 mg/L). All had fasting low-density lipoprotein (LDL) cholesterol ≤ 130 mg/dL.
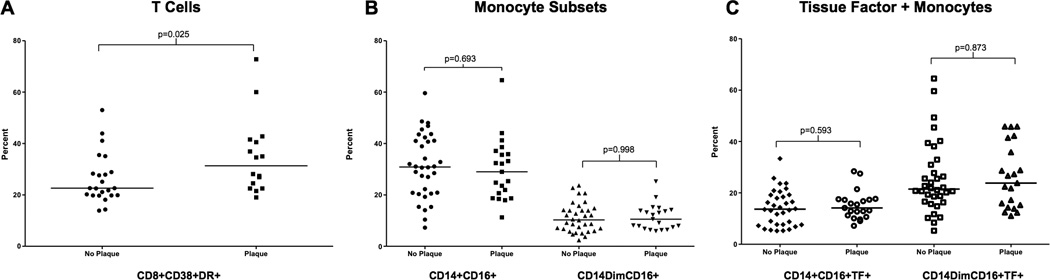
Results: Seventy-eight per cent of patients were men and 65% were African-American. Median (interquartile range) age and CD4 count were 47 (43, 52) years and 648 (511, 857) cells/μL, respectively. All had HIV-1 RNA < 400 HIV-1 RNA copies/mL. Mean CCA-IMT was correlated with log-transformed CD8(+)CD38(+)HLA-DR(+) percentage (r = 0.326; P = 0.043), and concentrations of interleukin-6 (r = 0.283; P = 0.028), soluble vascular cell adhesion molecule (sVCAM; r = 0.434; P = 0.004), tumour necrosis factor-α receptor-I (TNFR-I; r = 0.591; P < 0.0001) and fibrinogen (r = 0.257; P = 0.047). After adjustment for traditional cardiovascular disease (CVD) risk factors, the association with TNFR-I (P = 0.007) and fibrinogen (P = 0.033) remained significant. Subjects with plaque (n = 22; 37%) were older [mean (standard deviation) 51 (7.7) vs. 43 (9.4) years, respectively; P = 0.002], and had a higher CD8(+)CD38(+)HLA-DR(+) percentage [median (interquartile range) 31% (24, 41%) vs. 23% (20, 29%), respectively; P = 0.046] and a higher sVCAM concentration [mean (standard deviation) 737 (159) vs. 592 (160) ng/mL, respectively; P = 0.008] compared with those without plaque. Pro-inflammatory monocyte subsets and serum markers of monocyte activation (soluble CD163 and soluble CD14) were not associated with CCA-IMT or plaque.
Conclusions: Participants in SATURN-HIV have a high level of inflammation and immune activation that is associated with subclinical vascular disease despite low serum LDL cholesterol.
Trial registration: ClinicalTrials.gov NCT01218802.
© 2013 British HIV Association.
Figures
References
-
- Hulten E, Mitchell J, Scally J, Gibbs B, Villines TC. HIV positivity, protease inhibitor exposure and subclinical atherosclerosis: a systematic review and meta-analysis of observational studies. Heart. 2009 Nov;95(22):1826–1835. - PubMed
-
- Hsue PY, Giri K, Erickson S, MacGregor JS, Younes N, Shergill A, et al. Clinical features of acute coronary syndromes in patients with human immunodeficiency virus infection. Circulation. 2004 Jan 27;109(3):316–319. - PubMed
-
- Hsue PY, Hunt PW, Sinclair E, Bredt B, Franklin A, Killian M, et al. Increased carotid intima-media thickness in HIV patients is associated with increased cytomegalovirus-specific T-cell responses. Aids. 2006 Nov 28;20(18):2275–2283. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
