

Flecainide reduces Ca(2+) spark and wave frequency via inhibition of the sarcolemmal sodium current
- PMID: 23334259
- PMCID: PMC3714924
- DOI: 10.1093/cvr/cvt012
Flecainide reduces Ca(2+) spark and wave frequency via inhibition of the sarcolemmal sodium current
Abstract
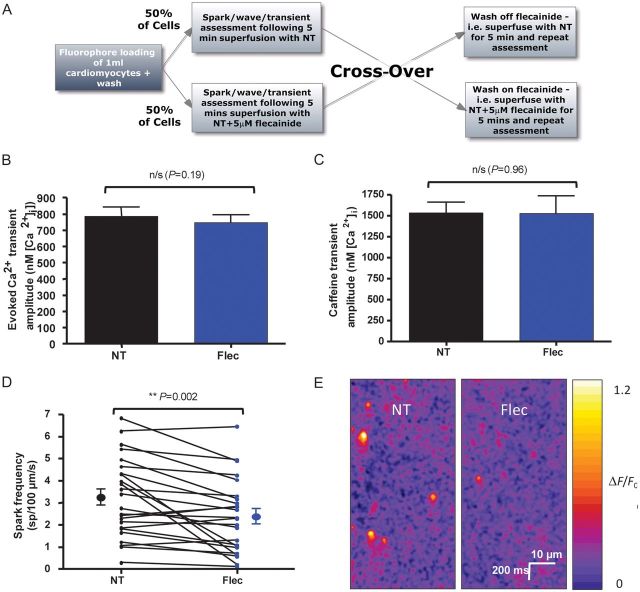
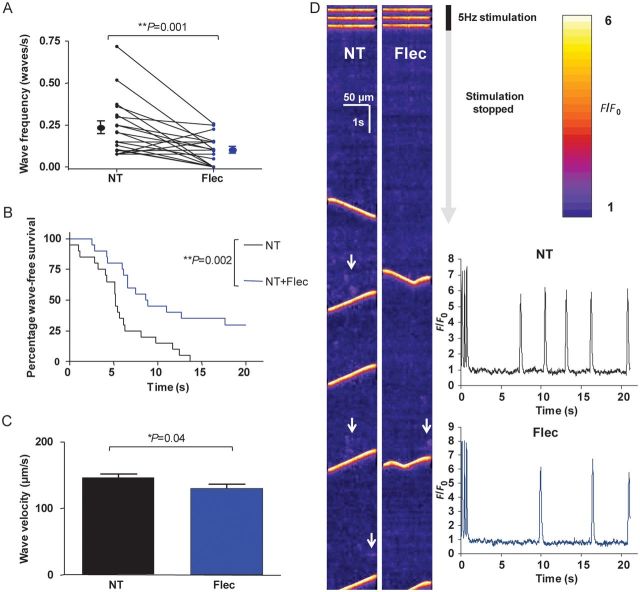
Aims: Ca(2+) waves are thought to be important in the aetiology of ventricular tachyarrhythmias. There have been conflicting results regarding whether flecainide reduces Ca(2+) waves in isolated cardiomyocytes. We sought to confirm whether flecainide inhibits waves in the intact cardiomyocyte and to elucidate the mechanism.
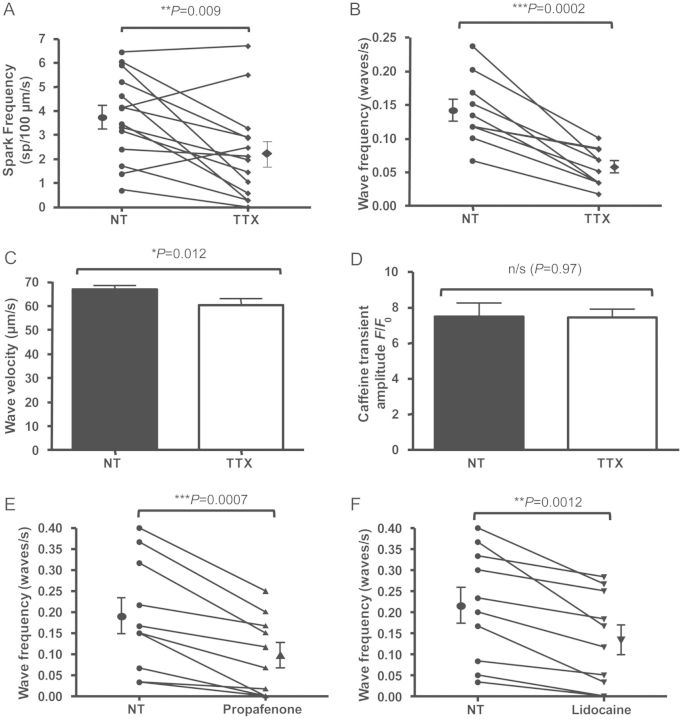
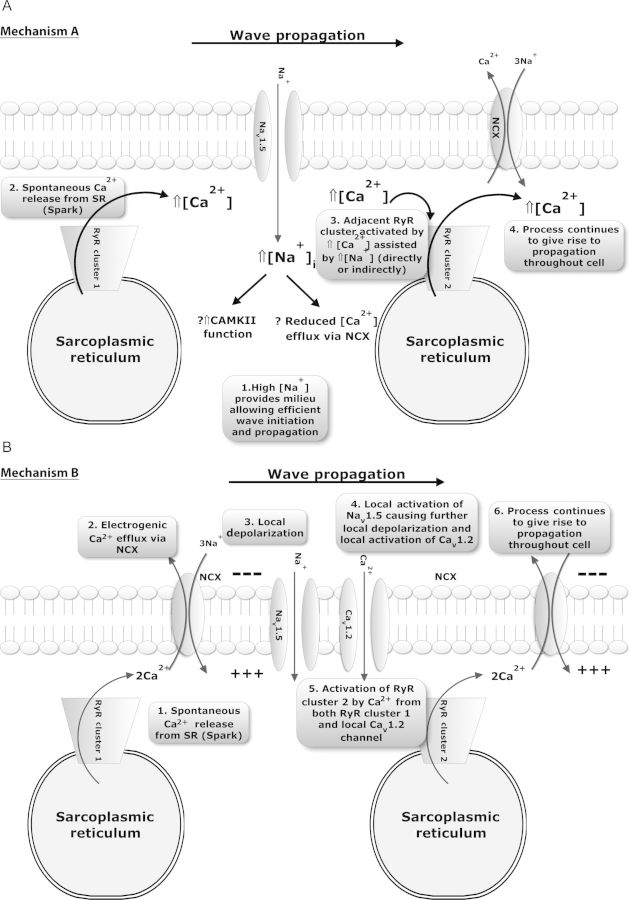
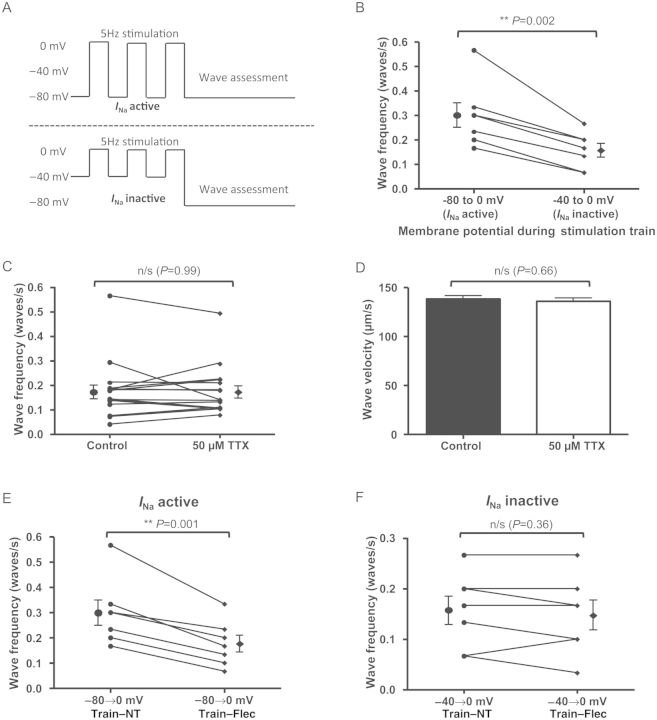
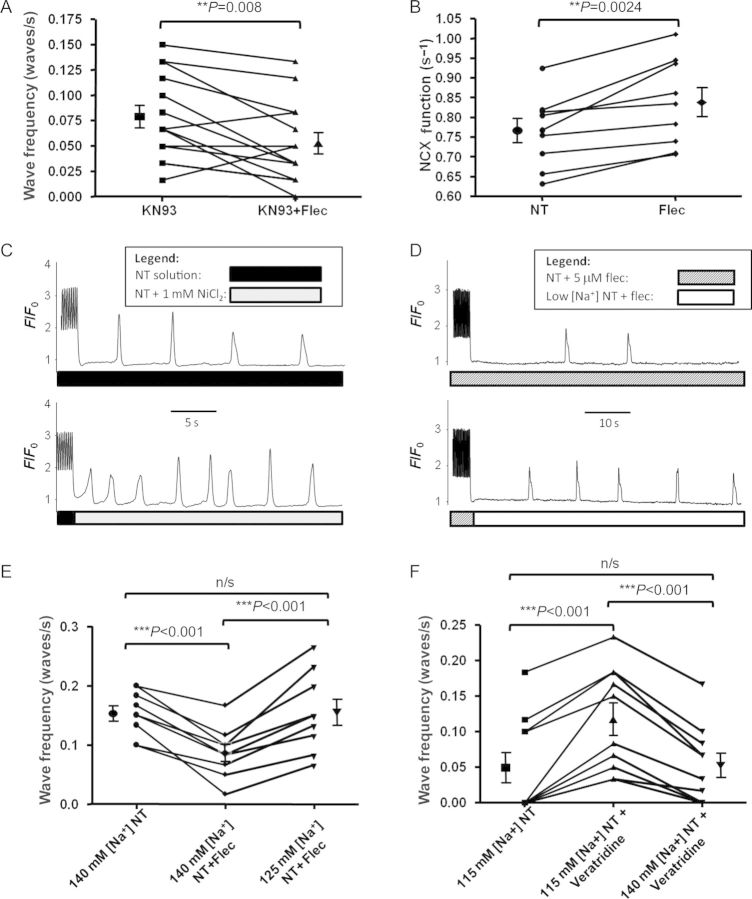
Methods and results: We imaged spontaneous sarcoplasmic reticulum (SR) Ca(2+) release events in healthy adult rat cardiomyocytes. Variation in stimulation frequency was used to produce Ca(2+) sparks or waves. Spark frequency, wave frequency, and wave velocity were reduced by flecainide in the absence of a reduction of SR Ca(2+) content. Inhibition of I(Na) via alternative pharmacological agents (tetrodotoxin, propafenone, or lidocaine) produced similar changes. To assess the contribution of I(Na) to spark and wave production, voltage clamping was used to activate contraction from holding potentials of -80 or -40 mV. This confirmed that reducing Na(+) influx during myocyte stimulation is sufficient to reduce waves and that flecainide only causes Ca(2+) wave reduction when I(Na) is active. It was found that Na(+)/Ca(2+)-exchanger (NCX)-mediated Ca(2+) efflux was significantly enhanced by flecainide and that the effects of flecainide on wave frequency could be reversed by reducing [Na(+)](o), suggesting an important downstream role for NCX function.
Conclusion: Flecainide reduces spark and wave frequency in the intact rat cardiomyocyte at therapeutically relevant concentrations but the mechanism involves I(Na) reduction rather than direct ryanodine receptor (RyR2) inhibition. Reduced I(Na) results in increased Ca(2+) efflux via NCX across the sarcolemma, reducing Ca(2+) concentration in the vicinity of the RyR2.
Figures
Comment in
-
Triple mode of action of flecainide in catecholaminergic polymorphic ventricular tachycardia.Cardiovasc Res. 2013 May 1;98(2):326-7. doi: 10.1093/cvr/cvt059. Epub 2013 Mar 19. Cardiovasc Res. 2013. PMID: 23512981 Free PMC article. No abstract available.
-
Triple mode of action of flecainide in catecholaminergic polymorphic ventricular tachycardia: reply.Cardiovasc Res. 2013 May 1;98(2):327-8. doi: 10.1093/cvr/cvt068. Epub 2013 Mar 27. Cardiovasc Res. 2013. PMID: 23536607 No abstract available.
References
-
- Zhou Q, Xiao J, Jiang D, Wang R, Vembaiyan K, Wang A, et al. Carvedilol and its new analogs suppress arrhythmogenic store overload-induced Ca2+ release. Nat Med. 2011;17:1003–1009. doi:10.1038/nm.2406. - DOI - PMC - PubMed
-
- Shannon TR, Pogwizd SM, Bers DM. Elevated sarcoplasmic reticulum Ca2+ leak in intact ventricular myocytes from rabbits in heart failure. Circ Res. 2003;93:592–594. doi:10.1161/01.RES.0000093399.11734.B3. - DOI - PubMed
-
- Lyon AR, Bannister ML, Collins T, Pearce E, Sepehripour AH, Dubb SS, et al. SERCA2a gene transfer decreases sarcoplasmic reticulum calcium leak and reduces ventricular arrhythmias in a model of chronic heart failure. Circ Arrhythm Electrophysiol. 2011;4:362–372. doi:10.1161/CIRCEP.110.961615. - DOI - PMC - PubMed
-
- MacLennan DH, Chen SR. Store overload-induced Ca2+ release as a triggering mechanism for CPVT and MH episodes caused by mutations in RYR and CASQ genes. J Physiol. 2009;587:3113–3115. doi:10.1113/jphysiol.2009.172155. - DOI - PMC - PubMed
-
- Kushnir A, Marks AR. The ryanodine receptor in cardiac physiology and disease. Adv Pharmacol. 2010;59:1–30. doi:10.1016/S1054-3589(10)59001-X. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
