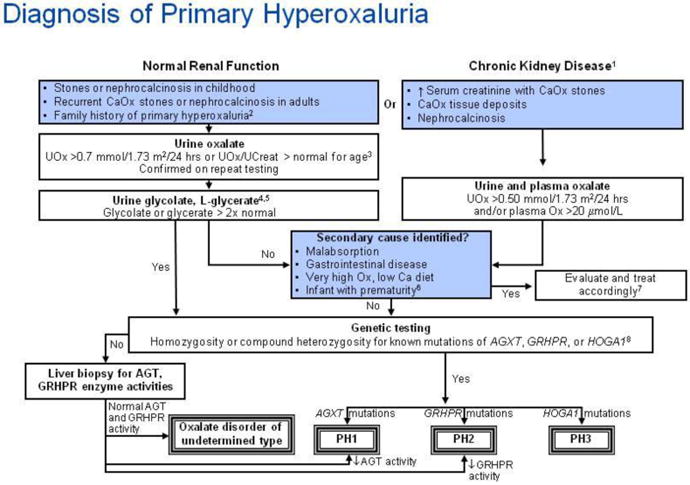
Algorithm for diagnostic evaluation of primary hyperoxaluria. Annotations to Figure 7
1Chronic kidney disease is defined as a glomerular filtration rate of less than 50 ml/min/1.73 m
2, or serum creatinine that is greater than or equal to two times normal for age.
2The guideline does not address prenatal diagnosis [121, 122].
3Urine oxalate-to-creatinine ratios in healthy children vary continuously by age. Tables of normal values should be consulted in interpretation of any random urine oxalate-to-creatinine ratio.
| Random urine oxalate-to-creatinine (Ox/Cr) ratio by age [123-126] |
| Age | Ox/Cr ratio Upper limit of normal |
| (mmol/mmol) | (mg/mg) |
| <6 months | 0.37 | 0.29 |
| 6 months to 2 years | 0.26 | 0.20 |
| >2 years to 5 years | 0.14 | 0.11 |
| 6 to 12 years | 0.08 | 0.063 |
Little data is available to guide interpretation of random urine oxalate-to-creatinine ratio in adolescents and adults. Upper limits of normal ratios declining to 0.04 by age 18-20 years and then remaining stable through adult age are suggested by available literature [125, 127]. In patients of all ages, confirmation of hyperoxaluria by a 24 hour urine collection with normalization of the oxalate excretion rate to 1.73 m
2 body surface area, is strongly recommended. From 2 years of age through adulthood, normal urine oxalate is constant at <0.45 mmol/1.73 m
2/24 hours [125].
4Urine and plasma oxalate and urine glycolate measurements for diagnostic testing should be obtained while the patient is not receiving pyridoxine or vitamin supplements.
5 Increased urine glycolate in the presence of hyperoxaluria is suggestive, but not diagnostic of primary hyperoxaluria (PH) type 1. Increased urine L-glycerate in a hyperoxaluric patient suggests PH type 2.
6Urine oxalate-to-creatinine ratios are higher in very premature infants than in term infants, especially when they are receiving parenteral nutrition containing amino acids. The ratio falls when premature infants are receiving only glucose and electrolyte solutions [128].
7When very high oxalate or low dietary calcium is suspected as the cause of the hyperoxaluria, the diet should be corrected and the urine oxalate remeasured for verification.
8In some cases with firm clinical diagnosis, only one mutation is found even after analysis for large rearrangements, suggesting that regulatory or deep intronic mutations may be the second, undetected mutation. In such cases, the finding of a single disease-associated mutation in the context of a typical phenotype supports the clinical diagnosis of PH.