

Alpha-synuclein pathology and axonal degeneration of the peripheral motor nerves innervating pharyngeal muscles in Parkinson disease
- PMID: 23334595
- PMCID: PMC3552335
- DOI: 10.1097/NEN.0b013e3182801cde
Alpha-synuclein pathology and axonal degeneration of the peripheral motor nerves innervating pharyngeal muscles in Parkinson disease
Abstract
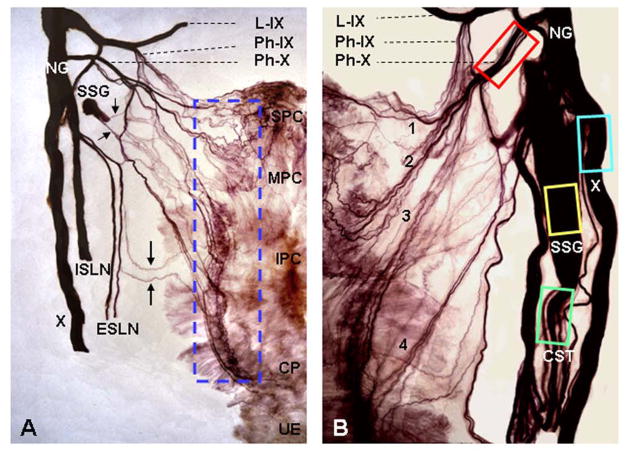
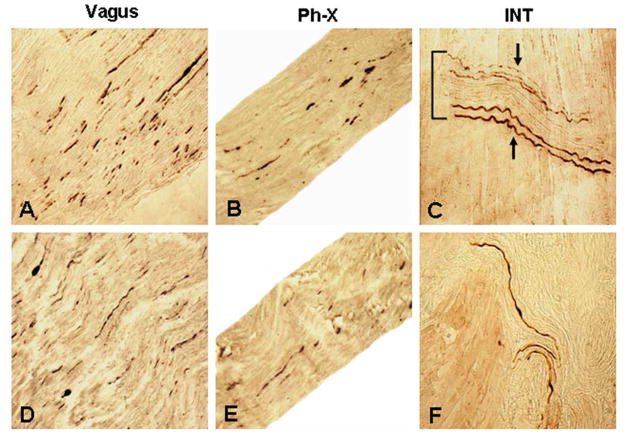
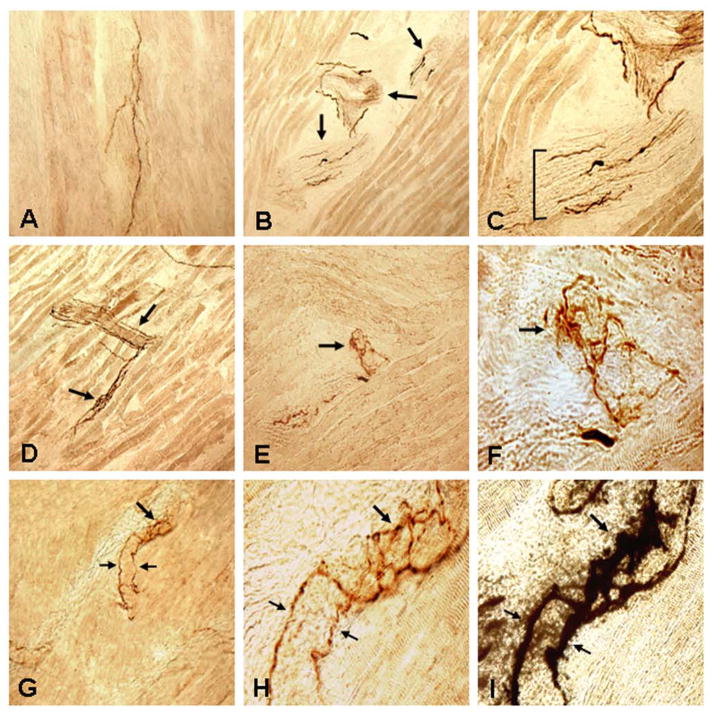
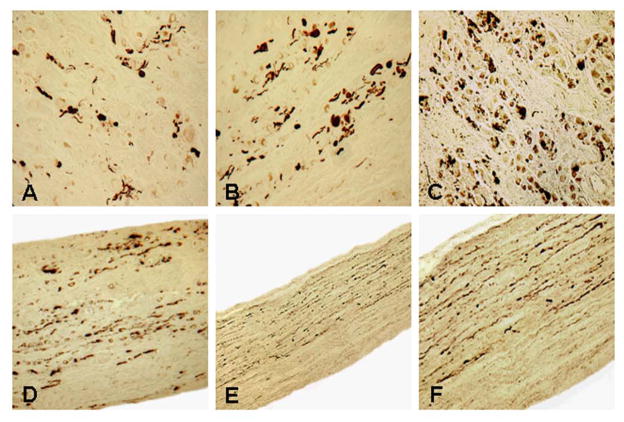
Parkinson disease (PD) is a neurodegenerative disease primarily characterized by cardinal motor manifestations and CNS pathology. Current drug therapies can often stabilize these cardinal motor symptoms, and attention has shifted to the other motor and nonmotor symptoms of PD that are resistant to drug therapy. Dysphagia in PD is perhaps the most important drug-resistant symptom because it leads to aspiration and pneumonia, the leading cause of death. Here, we present direct evidence for degeneration of the pharyngeal motor nerves in PD. We examined the cervical vagal nerve (cranial nerve X), pharyngeal branch of nerve X, and pharyngeal plexus innervating the pharyngeal muscles in 14 postmortem specimens, that is, from 10 patients with PD and 4 age-matched control subjects. Synucleinopathy in the pharyngeal nerves was detected using an immunohistochemical method for phosphorylated α-synuclein. Alpha-synuclein aggregates were revealed in nerve X and the pharyngeal branch of nerve X, and immunoreactive intramuscular nerve twigs and axon terminals within the neuromuscular junctions were identified in all of the PD patients but in none of the controls. These findings indicate that the motor nervous system of the pharynx is involved in the pathologic process of PD. Notably, PD patients who have had dysphagia had a higher density of α-synuclein aggregates in the pharyngeal nerves than those without dysphagia. These findings indicate that motor involvement of the pharynx in PD is one of the factors leading to oropharyngeal dysphagia commonly seen in PD patients.
Figures
References
-
- Jellinger KA. Pathology of Parkinson’s disease. Changes other than the nigrostriatal pathway. Mol Chem Neuropathol. 1991;14:153–97. - PubMed
-
- Johnston BT, Li Q, Castell JA, et al. Swallowing and esophageal function in Parkinson’s disease. Am J Gastroenterol. 1995;90:1741–46. - PubMed
-
- Leopold NA, Kagel MC. Prepharyngeal dysphagia in Parkinson’s disease. Dysphagia. 1996;11:14–22. - PubMed
-
- Coates C, Bakheit AM. Dysphagia in Parkinson’s disease. Eur Neurol. 1997;38:49–52. - PubMed
-
- Fuh JL, Lee RC, Wang SJ, et al. Swallowing difficulty in Parkinson’s disease. Clin Neurol Neurosurg. 1997;99:106–12. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
