

Combined ossification of the posterior longitudinal ligament at C2-3 and invagination of the posterior axis resulting in myelopathy
- PMID: 23334684
- PMCID: PMC3641260
- DOI: 10.1007/s00586-012-2654-8
Combined ossification of the posterior longitudinal ligament at C2-3 and invagination of the posterior axis resulting in myelopathy
Abstract
Purpose: Spinal stenosis at the C2-3 segment is a rare occurrence, and when it occurs myelopathy infrequently results. Furthermore, only a handful of cases involving congenital abnormalities of the posterior arch of the axis have been described resulting in cervical myelopathy many of which described simultaneous congenital abnormalities at adjacent levels and none of which identified ossification of the posterior longitudinal ligament (OPLL) at the same level. We report a case of a previously undescribed combination of abnormalities at the C2-3 segment resulting in clinical myelopathy.
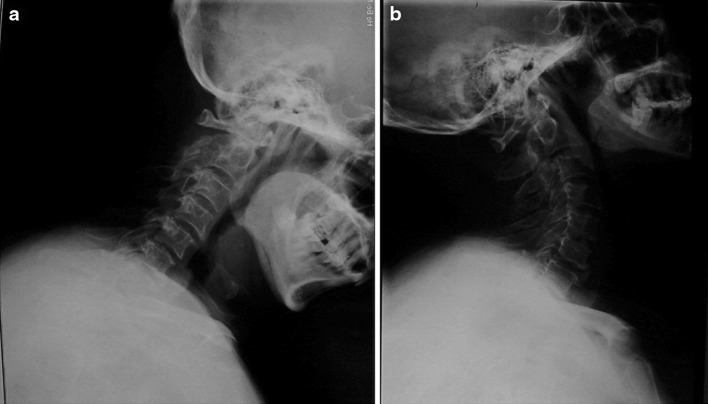
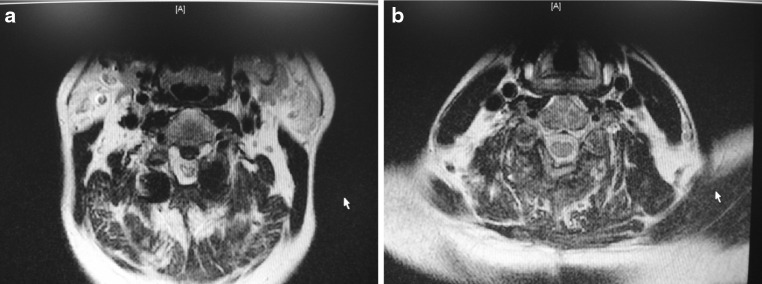
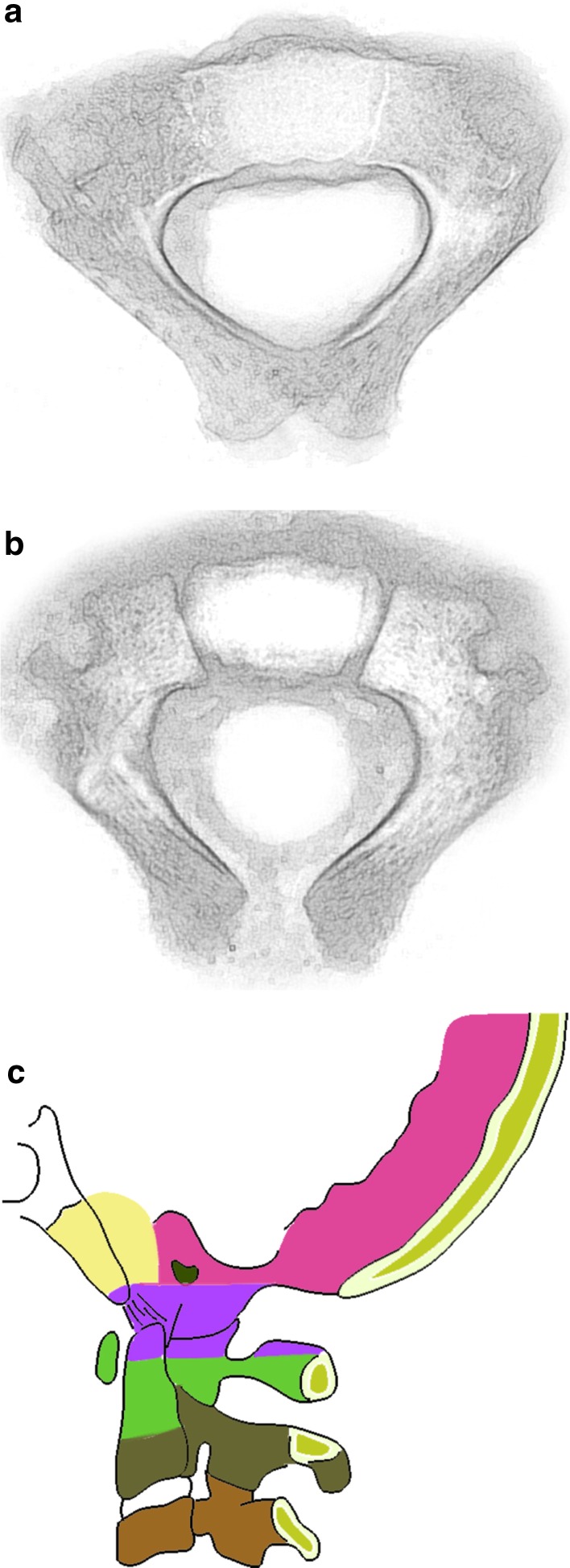
Methods: A 49-year-old Chinese male presented with a progressive cervical myelopathy (C-JOA score 11 immediately pre-op). Segmental OPLL at the C2-3 disk space was visible, together with invagination of the bilaterally hypoplastic C2 lamina into the spinal canal. Signal abnormalities of the spinal cord were evident on both T1 and T2 sequences.
Results: The patient underwent a posterior decompression and instrumented fusion at C2-3 using pars screws at C2 and lateral mass screws at C3. Following surgery there was a rapid and significant improvement in the neurological symptoms, with the C-JOA score improving to 14 at final follow-up. A successful fusion was evident.
Conclusions: Deficiencies in the posterior arch of the axis are rare and have not previously been reported in conjunction with OPLL. Advanced imaging is helpful to define the abnormality and site of compression. In the setting of a progressive neurological dysfunction, surgical decompression and stabilization is a reasonable intervention and can be associated with neurological and symptomatic improvement.
Figures





References
-
- Goel A, Gupta S, Laheri V. Congenital absence of posterior elements of axis: a report of two cases. Br J Neurosurg. 1999;13:459–461. - PubMed
-
- Behari S, Kiran Kumar MV, Banerji D, Chhabra DK, Jain VK. Atlantoaxial dislocation associated with the maldevelopment of the posterior neural arch of axis causing compressive myelopathy. Neurol India. 2004;52:250–251. - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
