

Hyperbaric oxygen induces late neuroplasticity in post stroke patients--randomized, prospective trial
- PMID: 23335971
- PMCID: PMC3546039
- DOI: 10.1371/journal.pone.0053716
Hyperbaric oxygen induces late neuroplasticity in post stroke patients--randomized, prospective trial
Abstract
Background: Recovery after stroke correlates with non-active (stunned) brain regions, which may persist for years. The current study aimed to evaluate whether increasing the level of dissolved oxygen by Hyperbaric Oxygen Therapy (HBOT) could activate neuroplasticity in patients with chronic neurologic deficiencies due to stroke.
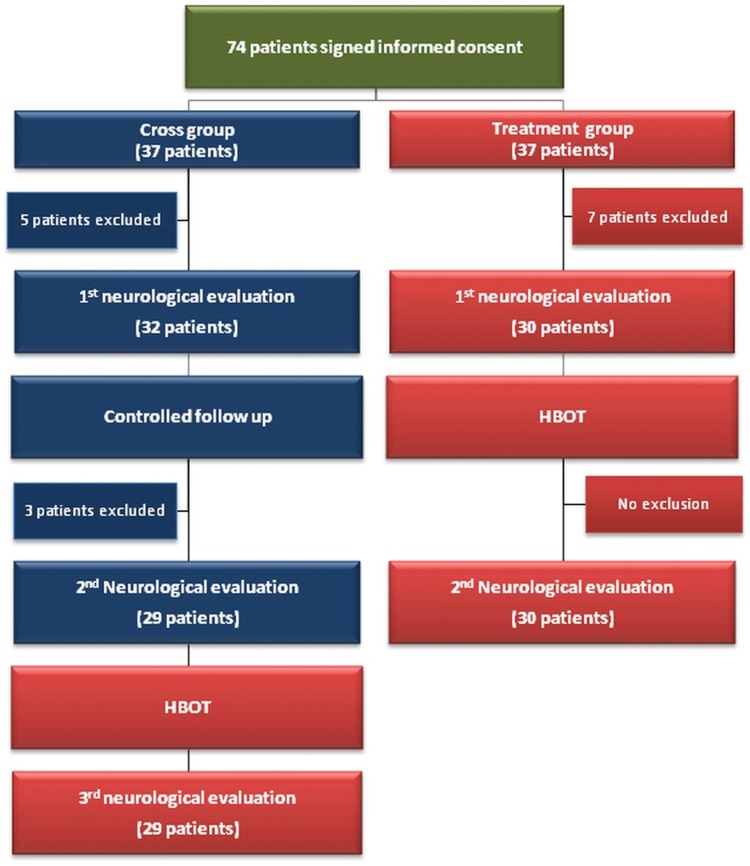
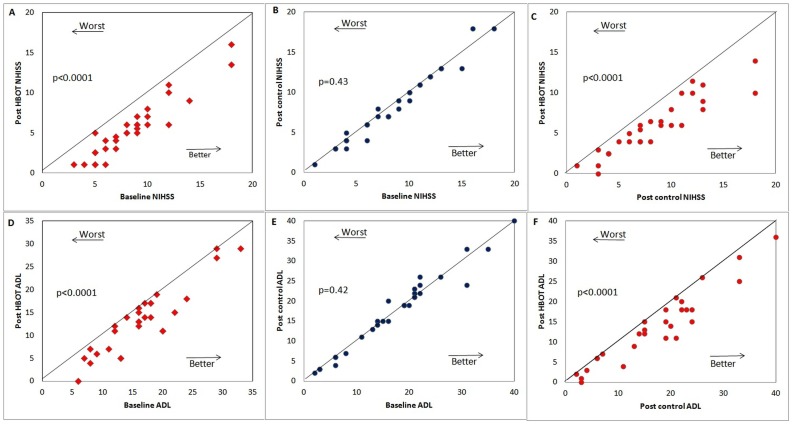
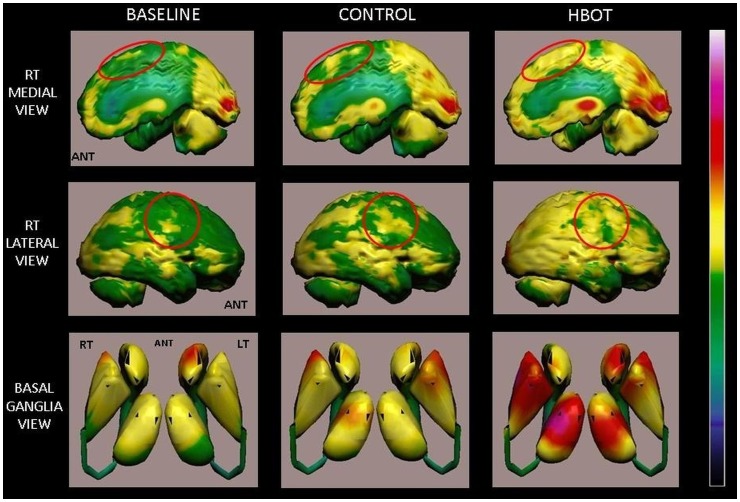
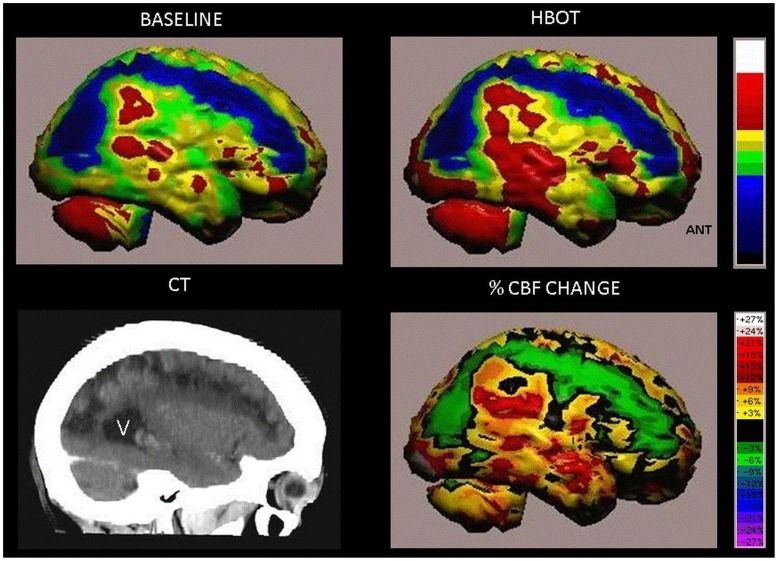
Methods and findings: A prospective, randomized, controlled trial including 74 patients (15 were excluded). All participants suffered a stroke 6-36 months prior to inclusion and had at least one motor dysfunction. After inclusion, patients were randomly assigned to "treated" or "cross" groups. Brain activity was assessed by SPECT imaging; neurologic functions were evaluated by NIHSS, ADL, and life quality. Patients in the treated group were evaluated twice: at baseline and after 40 HBOT sessions. Patients in the cross group were evaluated three times: at baseline, after a 2-month control period of no treatment, and after subsequent 2-months of 40 HBOT sessions. HBOT protocol: Two months of 40 sessions (5 days/week), 90 minutes each, 100% oxygen at 2 ATA. We found that the neurological functions and life quality of all patients in both groups were significantly improved following the HBOT sessions while no improvement was found during the control period of the patients in the cross group. Results of SPECT imaging were well correlated with clinical improvement. Elevated brain activity was detected mostly in regions of live cells (as confirmed by CT) with low activity (based on SPECT) - regions of noticeable discrepancy between anatomy and physiology.
Conclusions: The results indicate that HBOT can lead to significant neurological improvements in post stroke patients even at chronic late stages. The observed clinical improvements imply that neuroplasticity can still be activated long after damage onset in regions where there is a brain SPECT/CT (anatomy/physiology) mismatch.
Trial registration: ClinicalTrials.gov NCT00715897.
Conflict of interest statement
Figures


References
-
- Teasell R (2009) Forward. An international perspective of stroke rehabilitation. Top Stroke Rehabil 16: v. - PubMed
-
- Anderson DC, Bottini AG, Jagiella WM, Westphal B, Ford S, et al. (1991) A pilot study of hyperbaric oxygen in the treatment of human stroke. Stroke 22: 1137–1142. - PubMed
-
- Nighoghossian N, Trouillas P, Adeleine P, Salord F (1995) Hyperbaric oxygen in the treatment of acute ischemic stroke. A double-blind pilot study. Stroke; a journal of cerebral circulation 26: 1369–1372. - PubMed
-
- Rusyniak DE, Kirk MA, May JD, Kao LW, Brizendine EJ, et al. (2003) Hyperbaric oxygen therapy in acute ischemic stroke: results of the Hyperbaric Oxygen in Acute Ischemic Stroke Trial Pilot Study. Stroke; a journal of cerebral circulation 34: 571–574. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
