

Increased plasma sVCAM-1 is associated with severity in IgA nephropathy
- PMID: 23336423
- PMCID: PMC3557193
- DOI: 10.1186/1471-2369-14-21
Increased plasma sVCAM-1 is associated with severity in IgA nephropathy
Abstract
Background: A considerable proportion of IgAN patients present with histological vasculitic/crescentic lesions in glomeruli, indicating activation of vascular inflammation. Using sVCAM-1, a well-proven marker for endothelial injury under inflammatory processes, we investigated vascular injury and its association with clinical and pathological manifestations in IgAN patients.
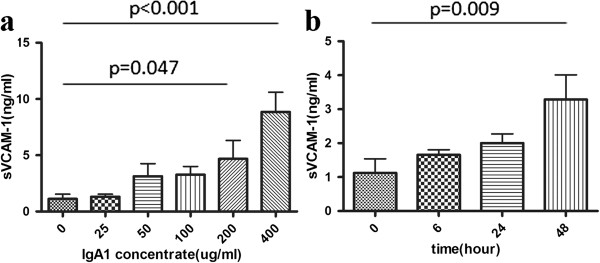
Methods: In this study, 327 biopsy-proven IgAN patients and 55 healthy controls were enrolled. The Oxford classification and two variables, Active Crescentic Lesion Percentage (ACLP) and Chronic Glomerular Lesion Percentage (CGLP), were used for evaluating pathological lesions. Human Umbilical Vein Endothelial Cells were treated with 25-400 ug/ml IgA1. sVCAM-1 in plasma and culture supernatant were measured by ELISA.
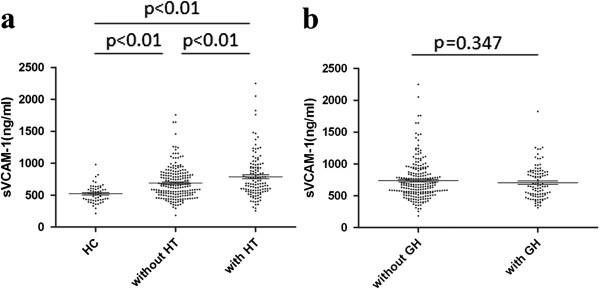
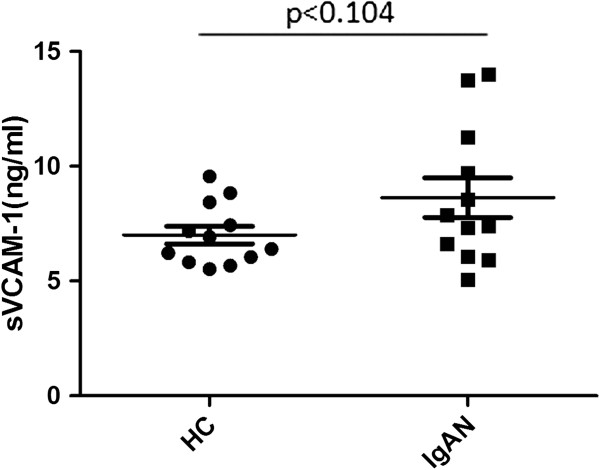
Results: Plasma sVCAM-1 in IgAN patients was significantly higher than healthy controls. In patients with IgAN, plasma sVCAM-1 was significantly correlated with eGFR, 24h urine protein excretion, tubular atrophy/interstitial fibrosis lesion and ACLP, but not CGLP. Meanwhile, compared to healthy volunteers, IgA1 from IgAN patients showed a tendency to increase the HUVECs supernatant sVCAM-1 expression. And IgA1 induced the sVCAM-1 increasing from HUVECs in time- and dose-dependent manner.
Conclusions: We found increased plasma sVCAM-1 in IgAN patients and its association with severe clinical and pathological manifestations, which might be partly resulted from effect of IgA1 to endothelial cells.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
