

A five-country evaluation of a point-of-care circulating cathodic antigen urine assay for the prevalence of Schistosoma mansoni
- PMID: 23339198
- PMCID: PMC3592520
- DOI: 10.4269/ajtmh.12-0639
A five-country evaluation of a point-of-care circulating cathodic antigen urine assay for the prevalence of Schistosoma mansoni
Abstract
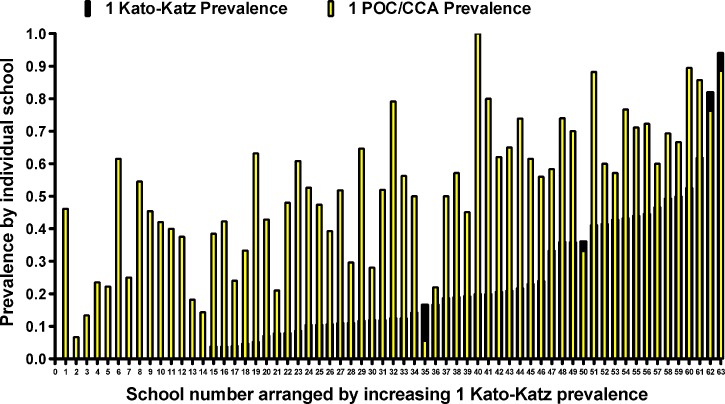
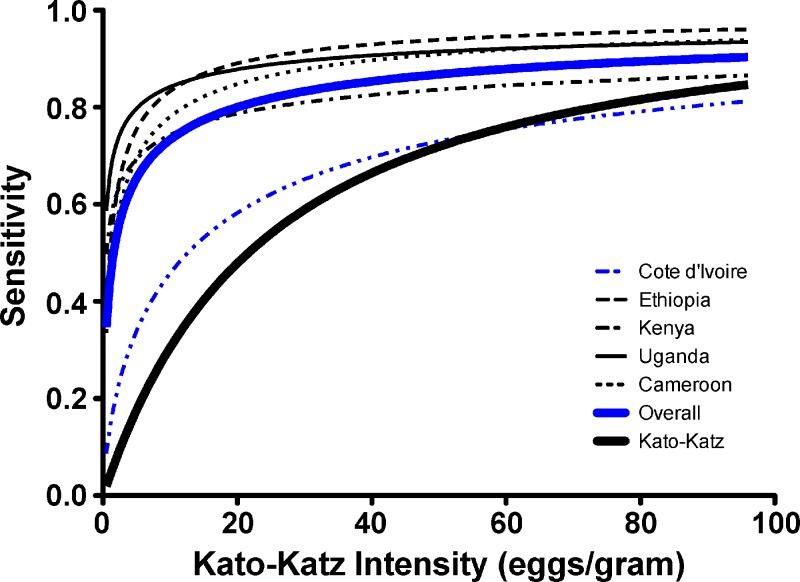
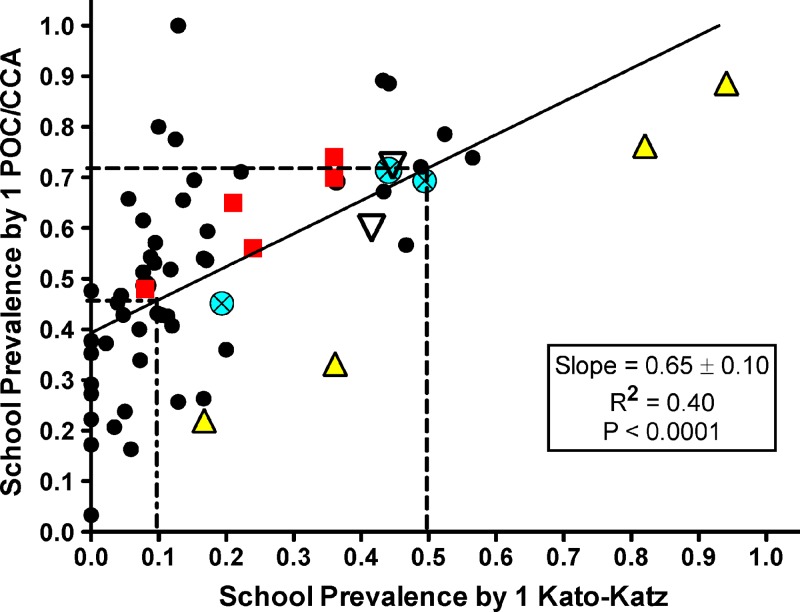
We evaluated a commercial point-of-care circulating cathodic antigen (POC-CCA) test for assessing Schistosoma mansoni infection prevalence in areas at risk. Overall, 4,405 school-age children in Cameroon, Côte d'Ivoire, Ethiopia, Kenya, and Uganda provided urine for POC-CCA testing and stool for Kato-Katz assays. By latent class analysis, one POC-CCA test was more sensitive (86% versus 62%) but less specific (72% versus ~100%) than multiple Kato-Katz smears from one stool. However, only 1% of POC-CCA tests in a non-endemic area were false positives, suggesting the latent class analysis underestimated the POC-CCA specificity. Multivariable modeling estimated POC-CCA as significantly more sensitive than Kato-Katz at low infection intensities (< 100 eggs/gram stool). By linear regression, 72% prevalence among 9-12 year olds by POC-CCA corresponded to 50% prevalence by Kato-Katz, whereas 46% POC-CCA prevalence corresponded to 10% Kato-Katz prevalence. We conclude that one urine POC-CCA test can replace Kato-Katz testing for community-level S. mansoni prevalence mapping.
Figures
References
-
- Katz N, Chaves A, Pellegrino J. A simple device for quantitative stool thick-smear technique in schistosomiasis mansoni. Rev Inst Med Trop Sao Paulo. 1972;14:397–400. - PubMed
-
- WHO . Preventive Chemotherapy in Human Helminthiasis: Coordinated Use of Anthelminthic Drugs in Control Interventions: A Manual For Health Professionals and Programme Managers. Geneva: World Health Organization; 2006.
-
- WHO . First WHO Report on Neglected Tropical Diseases 2010: Working to Overcome the Global Impact of Neglected Tropical Diseases. Geneva: World Health Organization; 2010.
-
- de Vlas SJ, Gryseels B. Underestimation of Schistosoma mansoni prevalences. Parasitol Today. 1992;8:274–277. - PubMed
-
- Utzinger J, Booth M, N'Goran EK, Muller I, Tanner M, Lengeler C. Relative contribution of day-to-day and intra-specimen variation in fecal egg counts of Schistosoma mansoni before and after treatment with praziquantel. Parasitology. 2001;122:537–544. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
