

Bone tissue engineering: recent advances and challenges
- PMID: 23339648
- PMCID: PMC3766369
- DOI: 10.1615/critrevbiomedeng.v40.i5.10
Bone tissue engineering: recent advances and challenges
Abstract
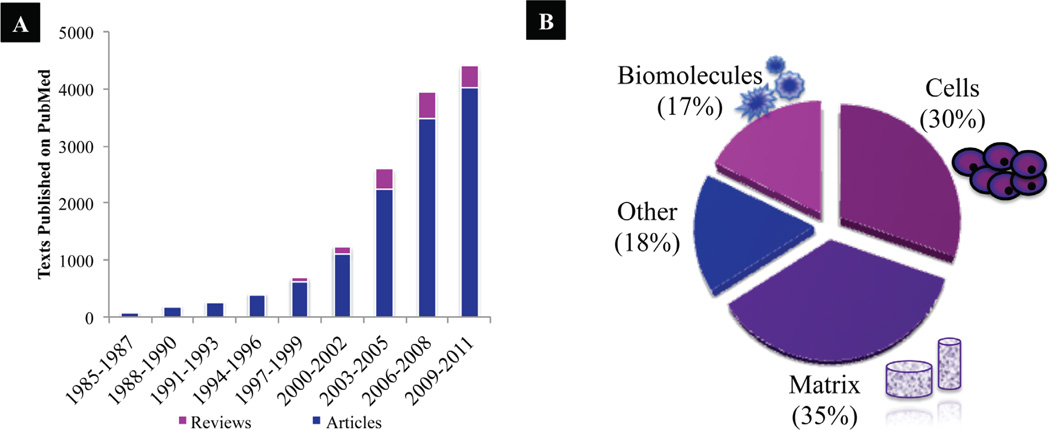
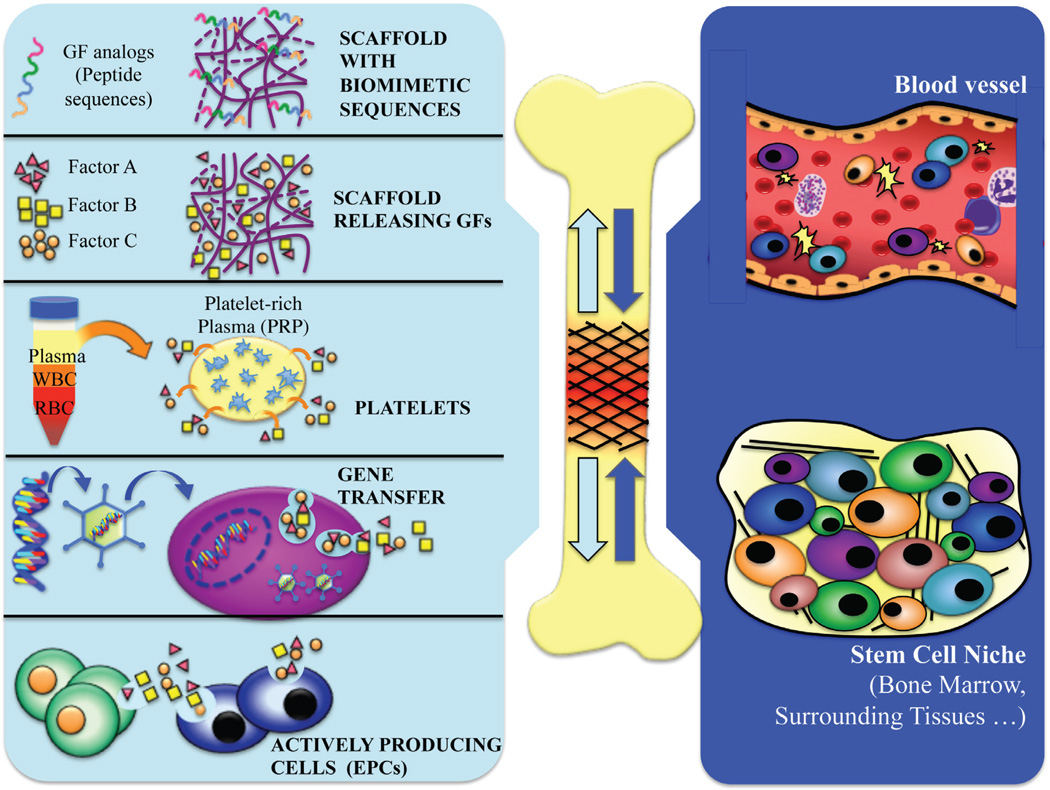
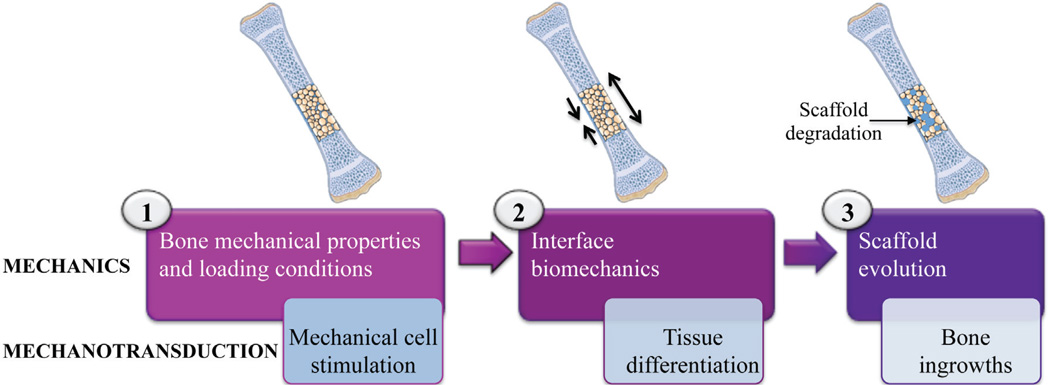
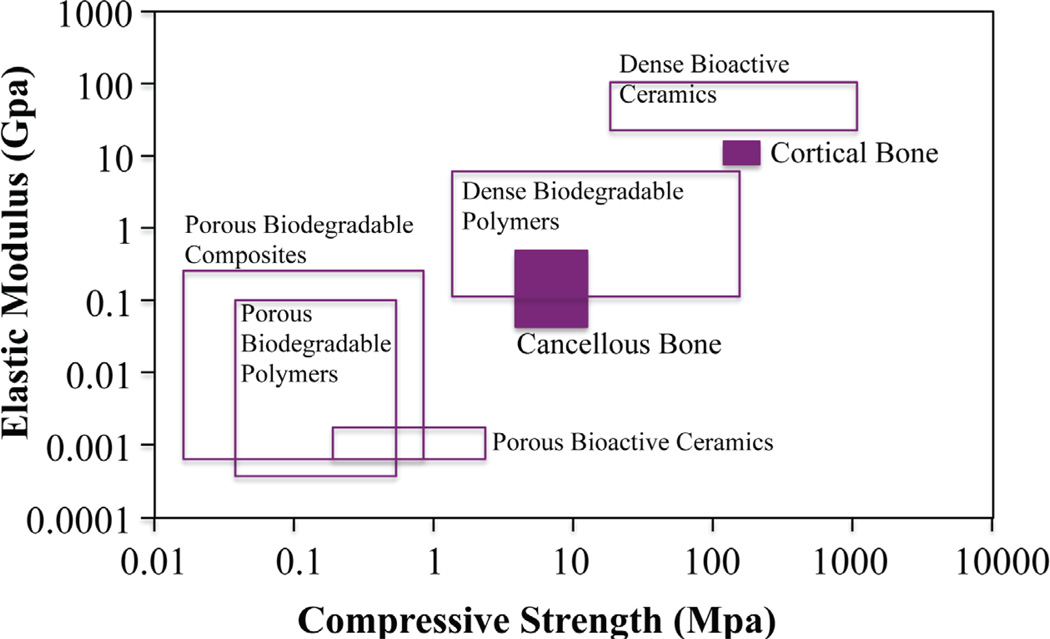
The worldwide incidence of bone disorders and conditions has trended steeply upward and is expected to double by 2020, especially in populations where aging is coupled with increased obesity and poor physical activity. Engineered bone tissue has been viewed as a potential alternative to the conventional use of bone grafts, due to their limitless supply and no disease transmission. However, bone tissue engineering practices have not proceeded to clinical practice due to several limitations or challenges. Bone tissue engineering aims to induce new functional bone regeneration via the synergistic combination of biomaterials, cells, and factor therapy. In this review, we discuss the fundamentals of bone tissue engineering, highlighting the current state of this field. Further, we review the recent advances of biomaterial and cell-based research, as well as approaches used to enhance bone regeneration. Specifically, we discuss widely investigated biomaterial scaffolds, micro- and nano-structural properties of these scaffolds, and the incorporation of biomimetic properties and/or growth factors. In addition, we examine various cellular approaches, including the use of mesenchymal stem cells (MSCs), embryonic stem cells (ESCs), adult stem cells, induced pluripotent stem cells (iPSCs), and platelet-rich plasma (PRP), and their clinical application strengths and limitations. We conclude by overviewing the challenges that face the bone tissue engineering field, such as the lack of sufficient vascularization at the defect site, and the research aimed at functional bone tissue engineering. These challenges will drive future research in the field.
Figures
References
-
- Laurencin CT, Ambrosio AM, Borden MD, Cooper JA. Tissue engineering: orthopedic applications. Annu Rev Biomed Eng. 1999;1:19–46. - PubMed
-
- Laurencin CT, Khan Y, El-Amin SF. Bone graft substitutes. Expert Rev Med Devices. 2006;3(1):49–57. - PubMed
-
- Nukavarapu SP, Wallace J, Elgendy H, Lieberman J, Laurencin CT. Bone and biomaterials. In: group TF, editor. An introduction to biomaterials and their applications. 2 ed. CRC Press; 2011. pp. 571–593.
-
- Baroli B. From natural bone grafts to tissue engineering therapeutics: brainstorming on pharmaceutical formulative requirements and challenges. J Pharm Sci. 2009;98(4):1317–1375. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials