

National Institutes of Health chronic graft-versus-host disease staging in severely affected patients: organ and global scoring correlate with established indicators of disease severity and prognosis
- PMID: 23340040
- PMCID: PMC3619213
- DOI: 10.1016/j.bbmt.2013.01.013
National Institutes of Health chronic graft-versus-host disease staging in severely affected patients: organ and global scoring correlate with established indicators of disease severity and prognosis
Abstract
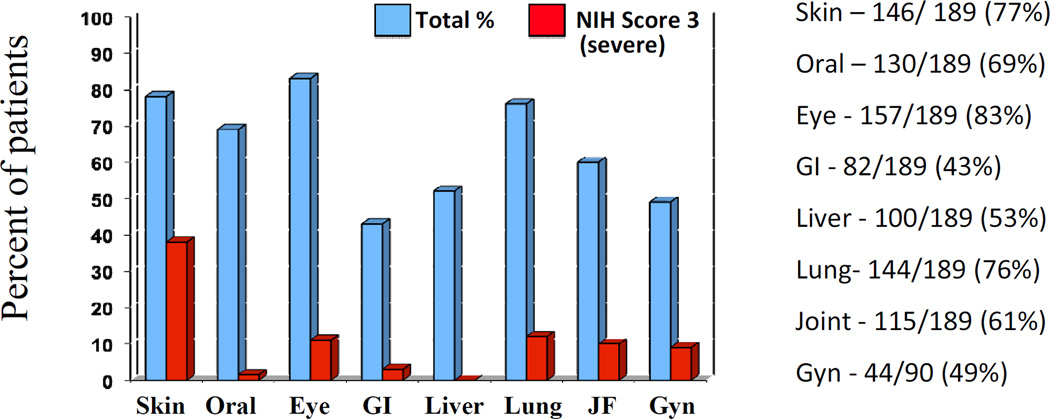
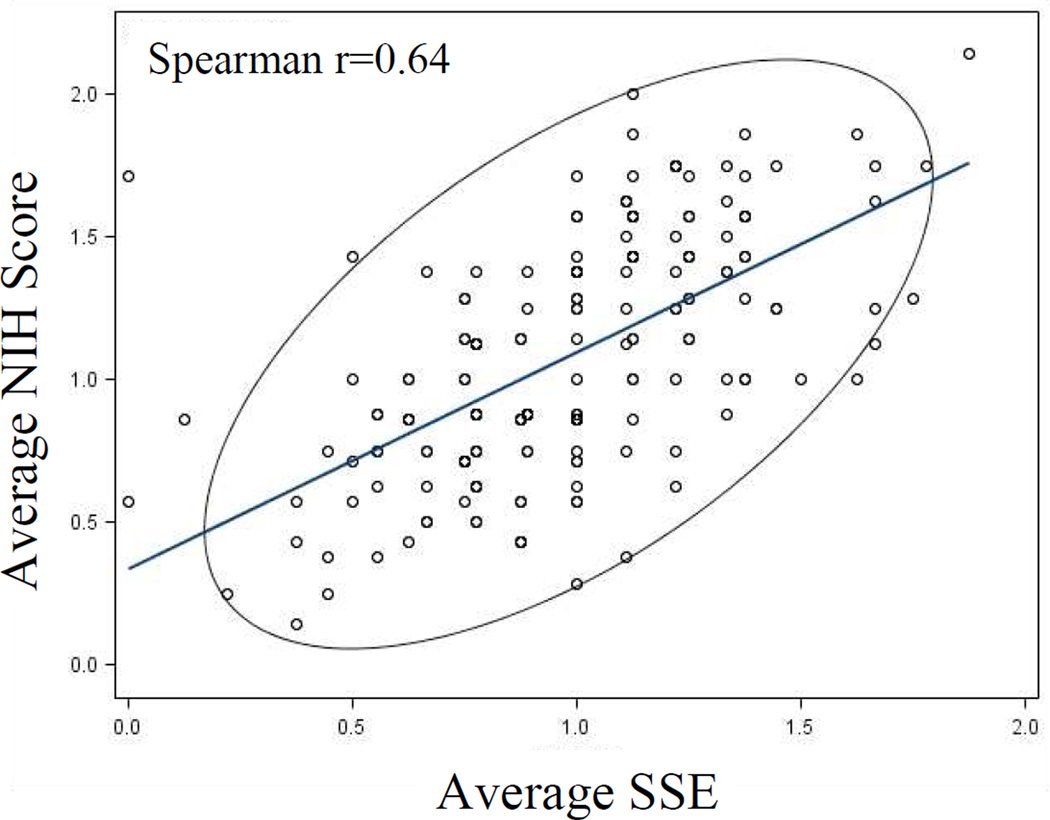
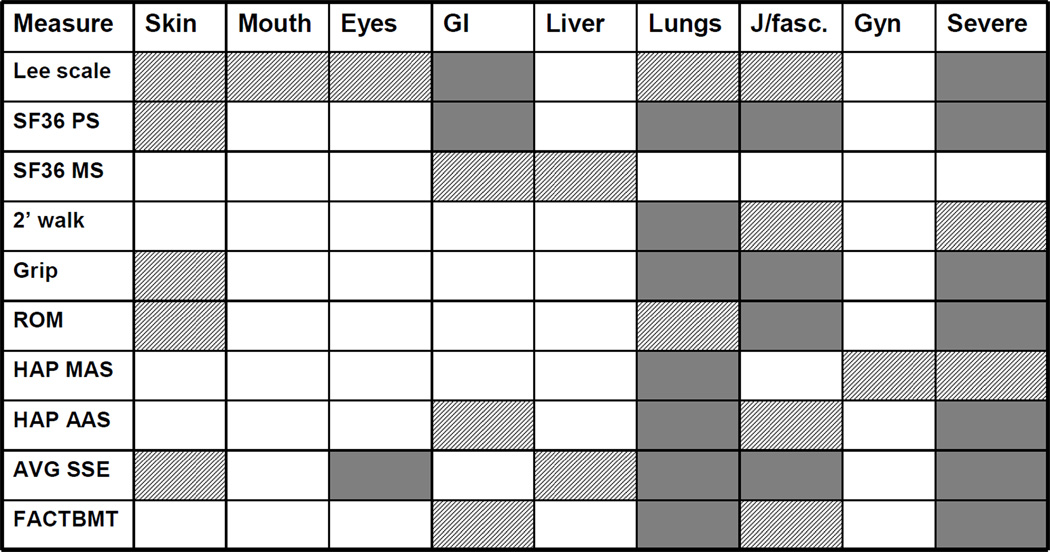
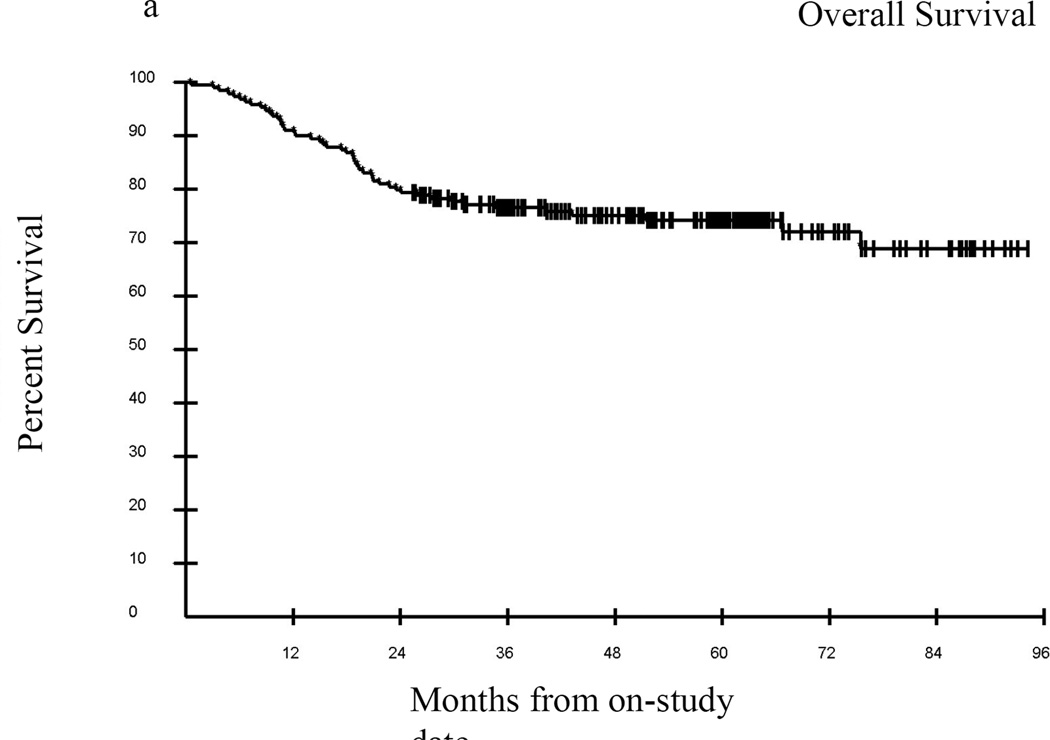
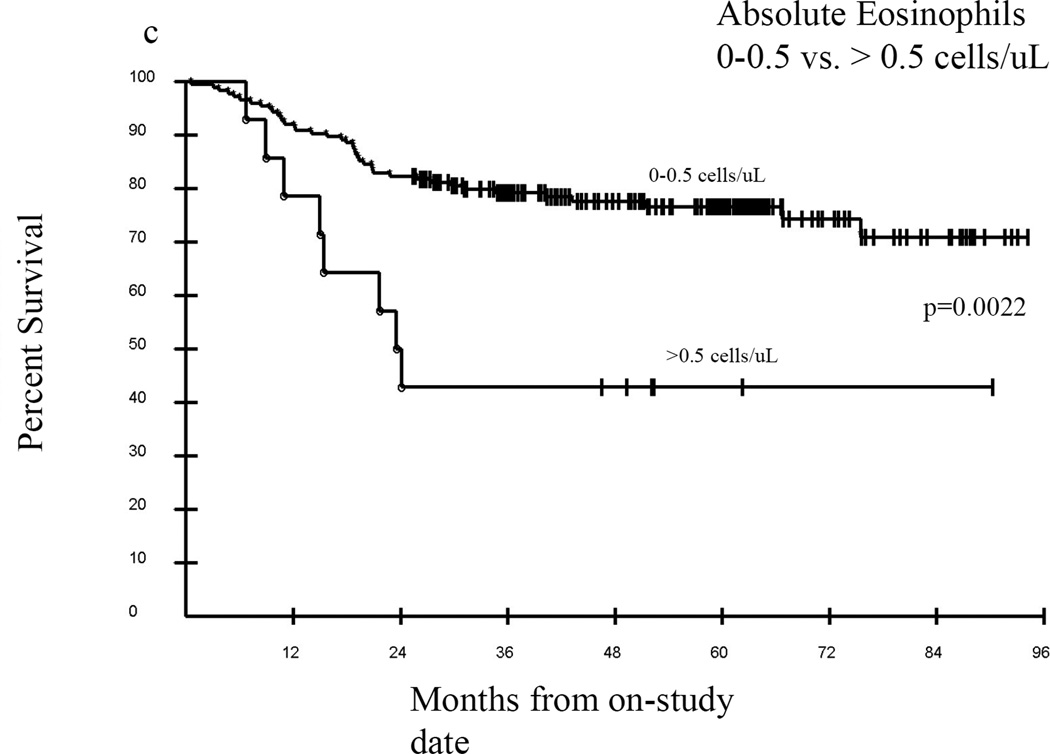
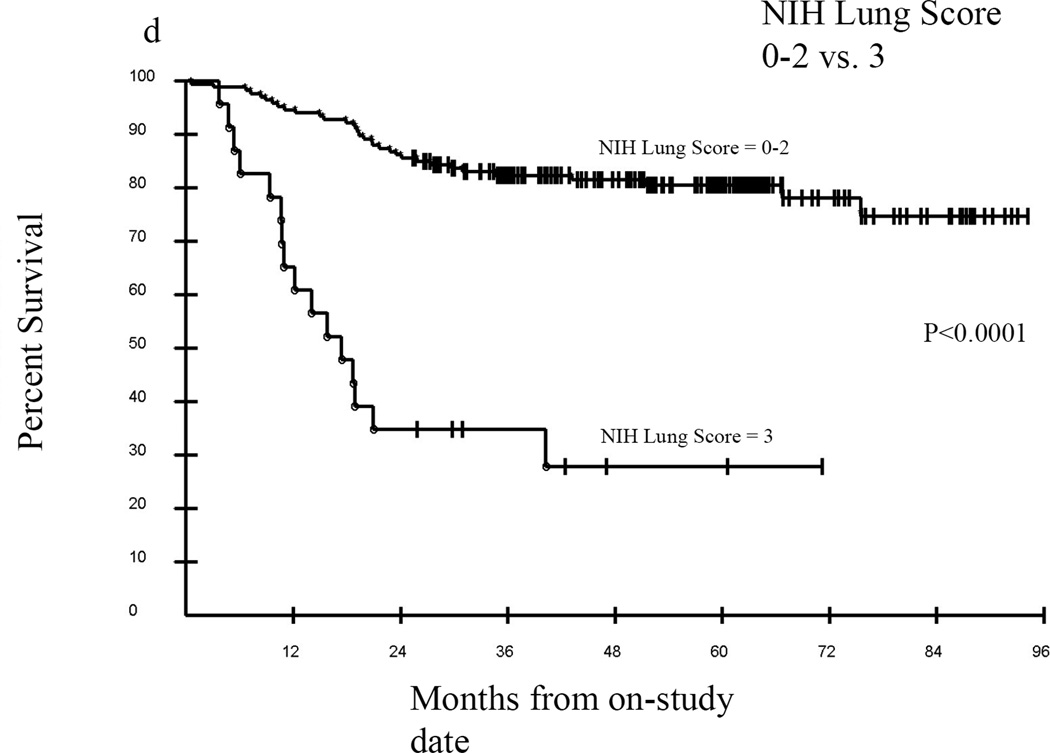
Between 2004 and 2010, 189 adult patients were enrolled on the National Cancer Institute's cross-sectional chronic graft-versus-host disease (cGVHD) natural history study. Patients were evaluated by multiple disease scales and outcome measures, including the 2005 National Institutes of Health (NIH) Consensus Project cGVHD severity scores. The purpose of this study was to assess the validity of the NIH scoring variables as determinants of disease severity in severely affected patients in efforts to standardize clinician evaluation and staging of cGVHD. Out of 189 patients enrolled, 125 met the criteria for severe cGVHD on the NIH global score, 62 of whom had moderate disease, with a median of 4 (range, 1-8) involved organs. Clinician-assigned average NIH organ score and the corresponding organ scores assigned by subspecialists were highly correlated (r = 0.64). NIH global severity scores showed significant associations with nearly all functional and quality of life outcome measures, including the Lee Symptom Scale, Short Form-36 Physical Component Scale, 2-minute walk, grip strength, range of motion, and Human Activity Profile. Joint/fascia, skin, and lung involvement affected function and quality of life most significantly and showed the greatest correlation with outcome measures. The final Cox model with factors jointly predictive for survival included the time from cGVHD diagnosis (>49 versus ≤49 months, hazard ratio [HR] = 0.23; P = .0011), absolute eosinophil count at the time of NIH evaluation (0-0.5 versus >0.5 cells/μL, HR = 3.95; P = .0006), and NIH lung score (3 versus 0-2, HR = 11.02; P < .0001). These results demonstrate that NIH organs and global severity scores are reliable measures of cGVHD disease burden. The strong association with subspecialist evaluation suggests that NIH organ and global severity scores are appropriate for clinical and research assessments, and may serve as a surrogate for more complex subspecialist examinations. In this population of severely affected patients, NIH lung score is the strongest predictor of poor overall survival, both alone and after adjustment for other important factors.
Published by Elsevier Inc.
Conflict of interest statement
The authors have no relevant conflicts to disclose.
Figures

References
-
- Lee SJ, Vogelsang G, Flowers ME. Chronic graft-versus-host disease. Biol Blood Marrow Transplant. 2003;9:215–233. - PubMed
-
- Carpenter PA. Late effects of chronic graft-versus-host disease. Best Pract Res Clin Haematol. 2008;21:309–331. - PubMed
-
- Arora M, Nagaraj S, Witte J, et al. New classification of chronic GVHD: added clarity from the consensus diagnoses. Bone Marrow Transplant. 2009;43:149–153. - PubMed
-
- Filipovich AH, Weisdorf D, Pavletic S, et al. National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: I. Diagnosis and Staging Working Group Report. Biol Blood Marrow Transplant. 2005;11:945–956. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
