

Reducing the frequency of acute otitis media by individualized care
- PMID: 23340550
- PMCID: PMC3681924
- DOI: 10.1097/INF.0b013e3182862b57
Reducing the frequency of acute otitis media by individualized care
Abstract
Objective: We sought to determine if use of more stringent diagnostic criteria for acute otitis media (AOM) than currently advocated by the American Academy of Pediatrics, tympanocentesis and pathogen-specific antibiotic treatment (individualized care) would result in reducing the incidence of recurrent AOM and consequent tympanostomy tube surgery.
Methods: A 5-year longitudinal, prospective study in Rochester, NY, was conducted from July 2006 to July 2011 involving 254 individualized care children. When this individualized care group developed symptoms of AOM, strict diagnostic criteria were applied and a tympanocentesis was performed. Pathogen resistance to empiric high-dose amoxicillin/clavulanate (80 mg/kg of amoxicillin component) caused a change in antibiotic to an optimized choice. Legacy controls (n = 208) were diagnosed with the same diagnostic criteria by the same physicians as the individualized care group and received the same empiric amoxicillin/clavulanate (80 mg/kg of amoxicillin component) but no tympanocentesis or change in antibiotic. Community control children (n = 1020) were diagnosed according to current American Academy of Pediatrics guidelines and treated with high-dose amoxicillin (80 mg/kg) without tympanocentesis as guideline recommended.
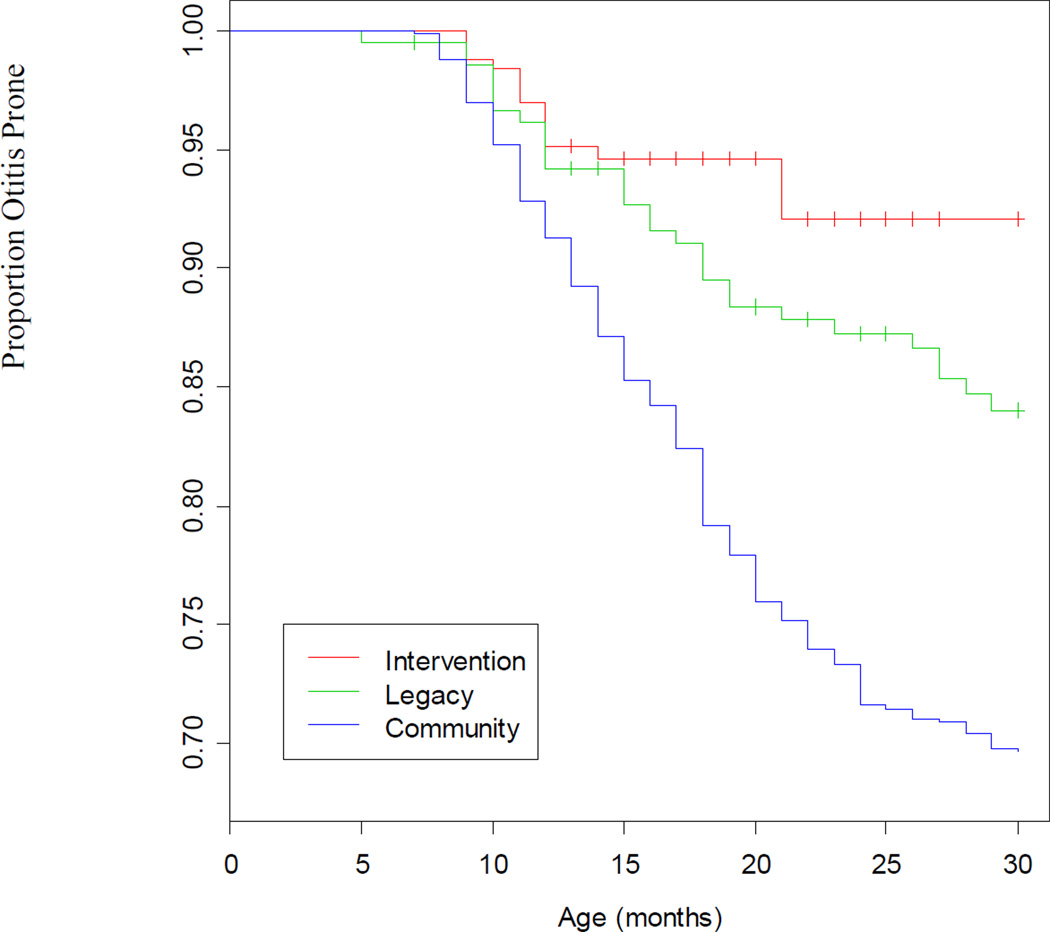
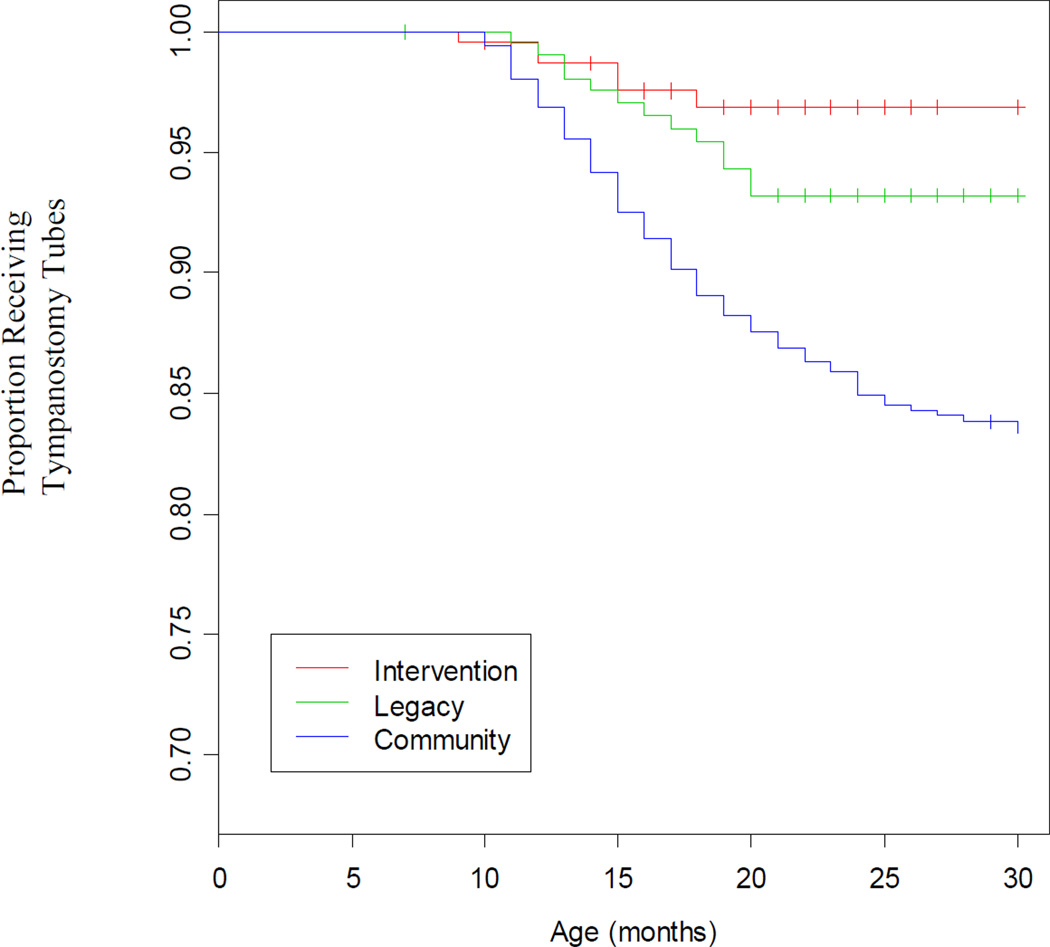
Results: 5.9% of children of the individualized care group compared with 14.4% of Legacy controls and 27.3% of community controls became otitis prone, defined as 3 episodes of AOM within a 6-month time span or 4 AOM episodes within a 12-month time span (P < 0.0001). 2.4% of the individualized care group compared with 6.3% of Legacy controls, and 14.8% of community controls received tympanostomy tubes (P < 0.0001).
Conclusions: Individualized care of AOM significantly reduces the frequency of AOM and tympanostomy tube surgery. Use of strict diagnostic criteria for AOM and empiric antibiotic treatment using evidence-based knowledge of circulating otopathogens and their antimicrobial susceptibility profile also produces improved outcomes.
Figures
References
-
- McCaig LF, Hughes JM. Trends in antimicrobial drug prescribing among office-based physicians in the United States. JAMA. 1995;273:214–219. - PubMed
-
- Pokras R, Kozak LJ, McCarthy E. Ambulatory and impatient procedures in the United States, 1994. Vital Health Stat 13. 1997;132:11–17. - PubMed
-
- Subcomittee on Management of Acute Otitis Media. Diagnosis and Management of Acute Otitis Media. Pediatrics. 2004;113:1451–1465. - PubMed
-
- The Otitis Media Guideline Panel. Managing otitis media with effusion in young children. Pediatrics. 1994;94:766–773. - PubMed
-
- Paradise JL, Feldman HM, Campbell TF, et al. Tympanostomy tubes and developmental outcomes at 9 to 11 years of age. N Engl J Med. 2007;356:248–261. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
