

Gliomatosis cerebri: clinical characteristics, management, and outcomes
- PMID: 23341100
- PMCID: PMC3907195
- DOI: 10.1007/s11060-013-1058-x
Gliomatosis cerebri: clinical characteristics, management, and outcomes
Abstract
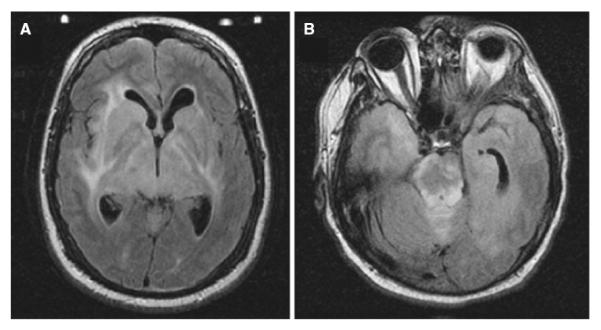
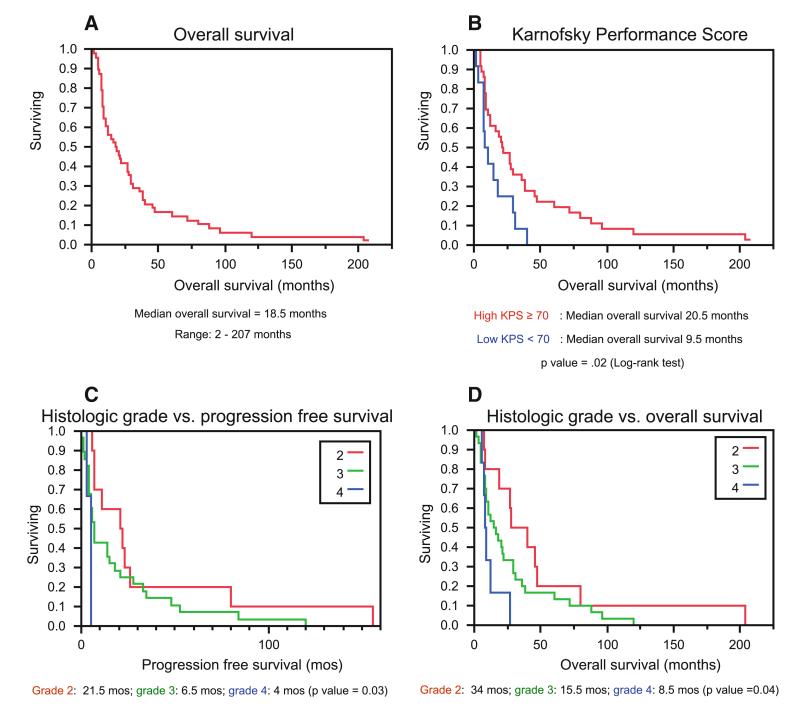
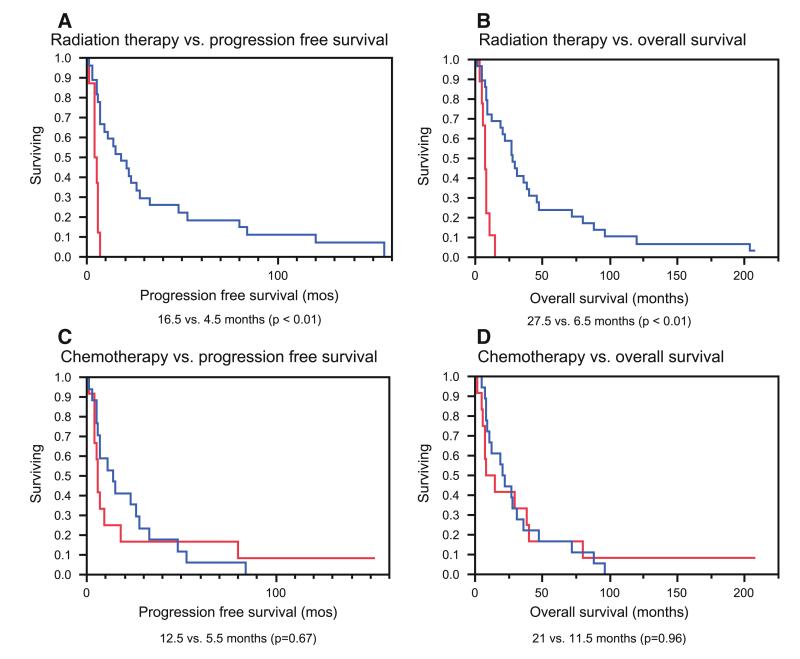
Gliomatosis cerebri is a rare diffusely infiltrating primary neoplastic glial process of the brain. Our objective is to review clinical presentation, management, and outcome in a large single institution series of gliomatosis cerebri patients. 54 consecutive gliomatosis cerebri cases presenting to Mayo Clinic Rochester between 1991 and 2008 were retrospectively reviewed. Inclusion criteria included involvement of at least three cerebral lobes, lack of a single discrete mass and pathological confirmation of diffuse glioma. Median overall survival (OS) was 18.5 months. Age, gender, presenting symptoms, and contrast enhancement did not correlate significantly with survival, though there was a trend toward decreased overall survival in patients above the median age of 46 years. Karnofsky performance score <70 was associated with poor OS (median 9.5 vs. 20.5 months, p = 0.02). Higher histologic grade was associated with poor progression-free survival (PFS; median for WHO grades II, III, and IV: 21.5, 6.5, and 4 months; p = 0.03) and OS (median 34, 15.5, and 8.5 months; p < 0.05). Radiation therapy was strongly associated with better prognosis (PFS 16.5 vs. 4.5 months, p < 0.01; OS 27.5 vs. 6.5, p < 0.01), but chemotherapy was not. Gliomatosis cerebri patients have a poor prognosis. Lower KPS upon presentation and higher histologic grade predict decreased survival. Surgery's role is limited beyond biopsy for diagnostic purposes. Radiotherapy appears beneficial, although selection bias could be present in this retrospective study. Chemotherapy's value is not as clear but this must be interpreted with caution given variable treatment regimens in this series.
Figures
References
-
- Couch JR, Weiss SA. Gliomatosis cerebri. Report of four cases and review of the literature. Neurology. 1974;24:504–511. - PubMed
-
- Kleihues P, Louis DN, Scheithauer BW, Rorke LB, Reifenberger G, Burger PC, Cavenee WK. The WHO classification of tumors of the nervous system. J Neuropathol Exp Neuro. 2002;61:226–229. - PubMed
-
- Artigas J, Cervos-Navarro J, Iglesias JR, Ebhardt G. Gliomatosis cerebri: clinical and histological findings. Clin Neuropathol. 1985;4:135–138. - PubMed
-
- Tans JT, de Jongh IE. Computed tomography of supratentorial astrocytoma. Clin Neurol Neurosurg. 1978;80:156–168. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
