

Prognostic usefulness of eosinopenia in the pediatric intensive care unit
- PMID: 23341721
- PMCID: PMC3546089
- DOI: 10.3346/jkms.2013.28.1.114
Prognostic usefulness of eosinopenia in the pediatric intensive care unit
Abstract
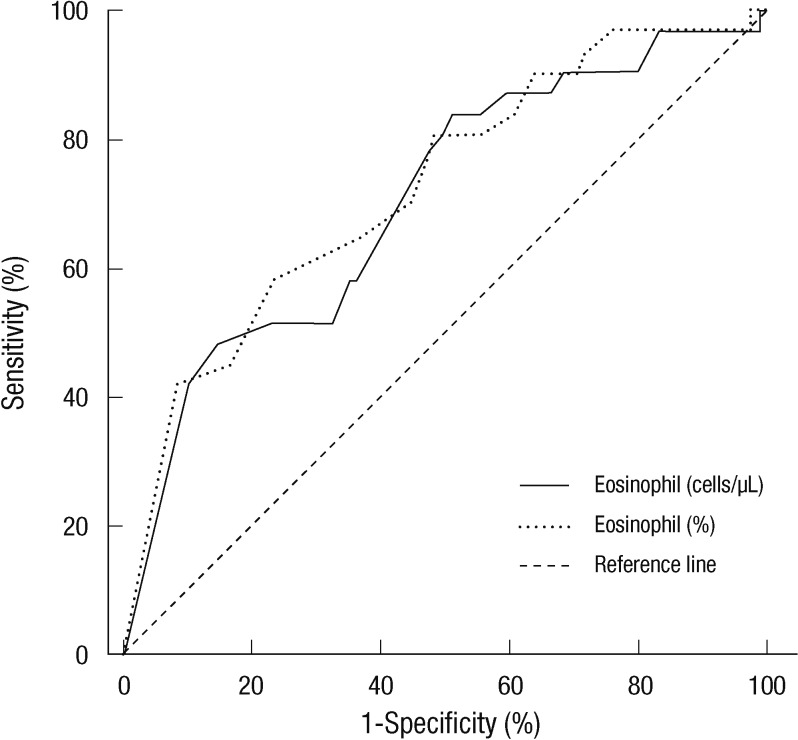
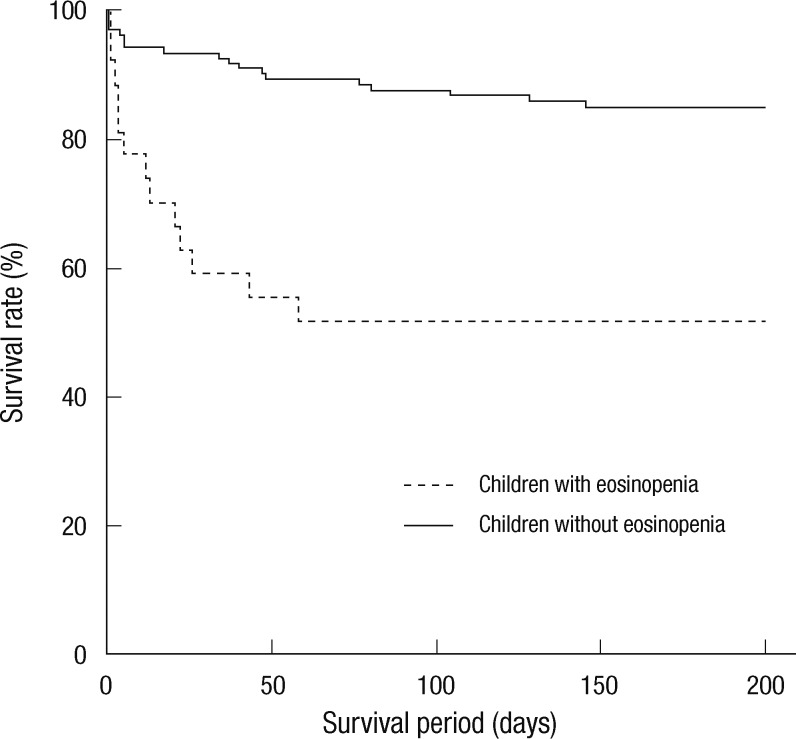
Eosinopenia, a biomarker for infection, has recently been shown to be a predictor of adult mortality in the intensive care unit (ICU). Our study assessed the usefulness of eosinopenia as a mortality and an infection biomarker in the pediatric ICU (PICU). We compared the PICU mortality scores, eosinophil count and percentage at ICU admission between children who survived and those who did not survive and between children with infection and those without infection. A total of 150 patients were evaluated. The initial eosinophil count and percentage were significantly lower in the group that did not survive when compared to those that did survive (P < 0.001; P < 0.001). However, there was no significant difference in the eosinophil count and percentage seen in patients with and without infection. Eosinopenia, defined as an eosinophil count < 15 cells/µL and an eosinophil percentage < 0.25%, (hazard ratio [HR]: 2.96; P = 0.008) along with a Pediatric Index of Mortality (PIM) 2 (HR: 1.03; P = 0.004) were both determined to be independent predictors of mortality in the PICU. The presence of eosinopenia at the ICU admission can be a useful biomarker for mortality in children, but is not useful as a biomarker for infection.
Keywords: Biomarkers; Child; Eosinophils; Infection; Intensive Care Units; Prognosis.
Figures
Similar articles
-
Eosinopenia, an early marker of increased mortality in critically ill medical patients.Intensive Care Med. 2011 Jul;37(7):1136-42. doi: 10.1007/s00134-011-2170-z. Epub 2011 Mar 3. Intensive Care Med. 2011. PMID: 21369810
-
Persistent eosinopenia is associated with in-hospital mortality among older patients: unexpected prognostic value of a revisited biomarker.BMC Geriatr. 2021 Oct 14;21(1):557. doi: 10.1186/s12877-021-02515-0. BMC Geriatr. 2021. PMID: 34649512 Free PMC article.
-
Eosinophil count (EC) as a diagnostic and prognostic marker for infection in the internal medicine department setting.Rom J Intern Med. 2019 Jun 1;57(2):166-174. doi: 10.2478/rjim-2018-0039. Rom J Intern Med. 2019. PMID: 30517081
-
[Eosinopenia in 2018].Rev Med Interne. 2019 Mar;40(3):173-177. doi: 10.1016/j.revmed.2018.11.008. Epub 2018 Nov 27. Rev Med Interne. 2019. PMID: 30501929 Review. French.
-
The role of eosinophils in sepsis and acute respiratory distress syndrome: a scoping review.Can J Anaesth. 2021 May;68(5):715-726. doi: 10.1007/s12630-021-01920-8. Epub 2021 Jan 25. Can J Anaesth. 2021. PMID: 33495945 Free PMC article.
Cited by
-
Evaluation of Eosinopenia as a SIRS Biomarker in Critically Ill Horses.Animals (Basel). 2022 Dec 15;12(24):3547. doi: 10.3390/ani12243547. Animals (Basel). 2022. PMID: 36552467 Free PMC article.
-
An Artificial Intelligence-guided signature reveals the shared host immune response in MIS-C and Kawasaki disease.Nat Commun. 2022 May 16;13(1):2687. doi: 10.1038/s41467-022-30357-w. Nat Commun. 2022. PMID: 35577777 Free PMC article.
-
Association between Eosinophil Count and Cortisol Concentrations in Equids Admitted in the Emergency Unit with Abdominal Pain.Animals (Basel). 2024 Jan 4;14(1):164. doi: 10.3390/ani14010164. Animals (Basel). 2024. PMID: 38200895 Free PMC article.
-
Eosinopenia Predicting Long-term Mortality in Hospitalized Acute Exacerbation of COPD Patients with Community-acquired Pneumonia-A Retrospective Analysis.Int J Chron Obstruct Pulmon Dis. 2021 Dec 30;16:3551-3559. doi: 10.2147/COPD.S347948. eCollection 2021. Int J Chron Obstruct Pulmon Dis. 2021. PMID: 35002227 Free PMC article.
-
C-Reactive Protein and Hemogram Parameters for the Non-Sepsis Systemic Inflammatory Response Syndrome and Sepsis: What Do They Mean?PLoS One. 2016 Feb 10;11(2):e0148699. doi: 10.1371/journal.pone.0148699. eCollection 2016. PLoS One. 2016. PMID: 26863002 Free PMC article.
References
-
- Kirkham FJ, Newton CR, Whitehouse W. Paediatric coma scales. Dev Med Child Neurol. 2008;50:267–274. - PubMed
-
- Lacroix J, Cotting J. Severity of illness and organ dysfunction scoring in children. Pediatr Crit Care Med. 2005;6:S126–S134. - PubMed
-
- Slater A, Shann F, Pearson G. PIM2: a revised version of the Paediatric Index of Mortality. Intensive Care Med. 2003;29:278–285. - PubMed
-
- Pollack MM, Patel KM, Ruttimann UE. PRISM III: an updated Pediatric Risk of Mortality score. Crit Care Med. 1996;24:743–752. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
