

Imaging and quantification of subbasal nerve plexus in healthy volunteers and diabetic patients with or without retinopathy
- PMID: 23341892
- PMCID: PMC3546080
- DOI: 10.1371/journal.pone.0052157
Imaging and quantification of subbasal nerve plexus in healthy volunteers and diabetic patients with or without retinopathy
Abstract
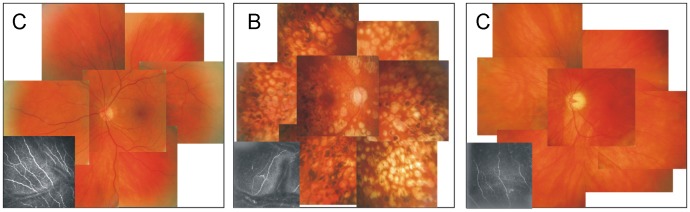
Background: The alterations of subbasal nerve plexus (SBP) innervation and corneal sensation were estimated non-invasively and compared with the values in healthy volunteers. Additionally, this study addressed the relation of SBP changes to the retinal status, glycemic control and diabetes duration.
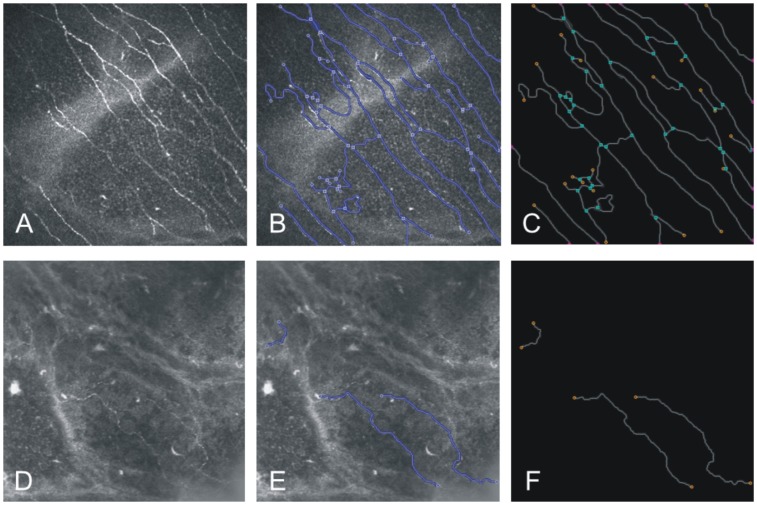
Methodology/principal findings: Eighteen eyes of diabetic patients with peripheral diabetic neuropathy aged 68.8±8.8 years and twenty eyes of healthy volunteers aged 66.3±13.3 yrs. were investigated with in vivo confocal laser-scanning microscopy (CLSM). An adapted algorithm for image analysis was used to quantify the morphological and topological properties of SBP. These properties were correlated to incidence of diabetic retinopathy (DR) and corneal sensation (Cochet-Bonnet esthesiometer). The developed algorithm allows a fully automated analysis of pre-segmented SBP structures. Altogether, 10 parameters were analysed, and all of them revealed significant differences between diabetic patients and healthy volunteers. The nerve fibre density, total fibre length and nerve branches were found to be significantly lower in patients with diabetes than those of control subjects (nerve fibre density 0.006±0.002 vs. 0.020±0.007 mm/mm(2); total fibre length 6223±2419 vs. 19961±6553 µm; nerve branches 25.3±28.6 vs. 141.9±85.7 in healthy volunteers). Also the corneal sensation was significantly lower in diabetic group when compared to controls (43±11 vs. 59±18 mm). There was found no difference in SBP morphology or corneal sensation in the subgroups with (DR) or without (NDR) diabetic retinopathy.
Conclusions/significance: SBP parameters were significantly reduced in diabetic patients, compared to control group. Interestingly, the SBP impairment could be shown even in the diabetic patients without DR. Although automatic adapted image analysis simplifies the evaluation of in vivo CLSM data, image acquisition and quantitative analysis should be optimised for the everyday clinical practice.
Conflict of interest statement
Figures
References
-
- Pirart J (1978) [Degenerative diabetic complications. Is persistent hyperglycemia more dangerous than wide glycemic fluctuations? (author's transl)]. Nouv Presse Med 7: 4031–4035. - PubMed
-
- Ziegler D, Zentai CP, Perz S, Rathmann W, Haastert B, et al. (2008) Prediction of mortality using measures of cardiac autonomic dysfunction in the diabetic and nondiabetic population: the MONICA/KORA Augsburg Cohort Study. Diabetes Care 31: 556–561. - PubMed
-
- MacDonald BK, Cockerell OC, Sander JW, Shorvon SD (2000) The incidence and lifetime prevalence of neurological disorders in a prospective community-based study in the UK. Brain 123 (Pt 4): 665–676. - PubMed
-
- Argoff CE, Cole BE, Fishbain DA, Irving GA (2006) Diabetic peripheral neuropathic pain: clinical and quality-of-life issues. Mayo Clin Proc 81: S3–11. - PubMed
-
- Vinik AI, Mehrabyan A (2004) Diabetic neuropathies. Med Clin North Am 88: 947–99, xi. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
