

Utility of NT-proBNP for identifying LV failure in patients with acute exacerbation of chronic bronchitis
- PMID: 23341901
- PMCID: PMC3544907
- DOI: 10.1371/journal.pone.0052553
Utility of NT-proBNP for identifying LV failure in patients with acute exacerbation of chronic bronchitis
Abstract
Background: NT-proBNP has been widely regarded as a useful tool for diagnosis or exclusion of heart failure (HF) in many settings. However, in patients with acute exacerbation of chronic bronchitis (AECB), its roles have not been well described. The objective of this study was to evaluate the diagnostic performance of NT-proBNP for identifying left ventricular (LV) failure in such patients.
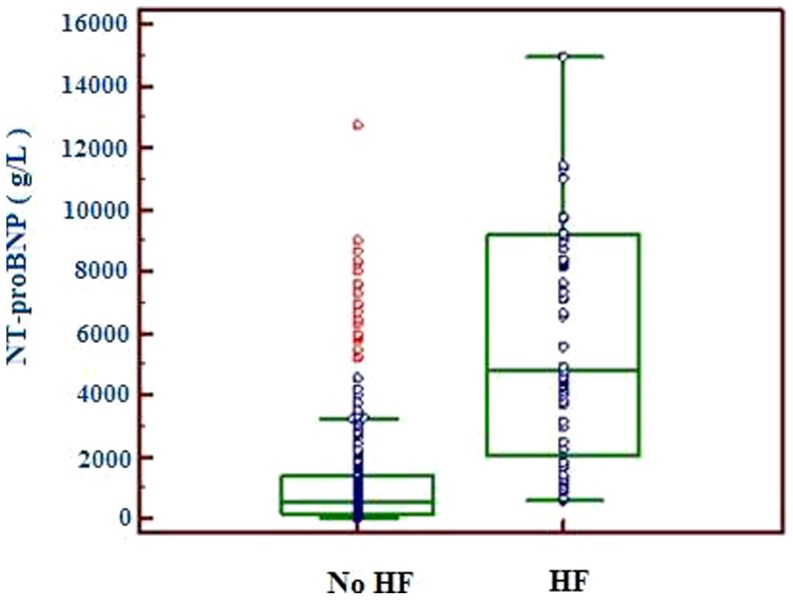
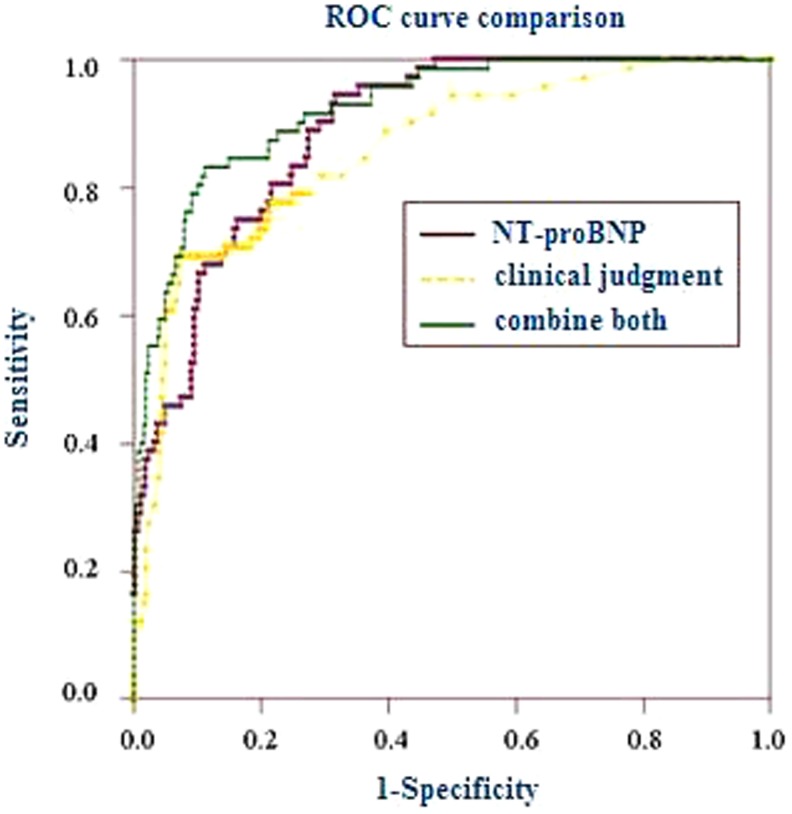
Methods and results: 311 AECB patients and 102 stable chronic bronchitis patients with no history of HF were enrolled. Plasma NT-proBNP concentrations were measured using Roche Elecsys. The European Society of Cardiology (ESC) diagnostic principles were adopted to identify HF and the diagnostic performance of NT-proBNP was evaluated by ROC. Our results showed, the median NT-proBNP level in patients with LV failure [4828.4 (2044.4-9203.6) ng/L] was significantly higher than that in those without LV failure [519.2 (179.1-1409.8) ng/L, p<0.001] and stable controls [207.5 (186.5-318.2) ng/L, p<0.001]. LV failure, renal function, atrial fibrillation and systolic pulmonary artery pressure were independent predictors of NT-proBNP levels (all p<0.05). The area under ROC curve (AUC) of NT-proBNP for identifying LV failure was 0.884, significantly superior to clinical judgment alone (AUC 0.835, p = 0.0294). At the optimal cutoff value of 935.0 ng/L, NT-proBNP yielded sensitivity 94.4%, specificity 68.2%, accuracy 74.3% and negative predictive value 97.6%. Adding the results of NT-proBNP to those of clinical judgment improved the diagnostic accuracy for LV failure.
Conclusion: As a tool for diagnosis or exclusion of HF, NT-proBNP can help physicians identify LV failure in patients with AECB.
Conflict of interest statement
Figures

Similar articles
-
Comparative value of BNP and NT-proBNP in diagnosis of heart failure.Rev Port Cardiol. 2004 Jul-Aug;23(7-8):979-91. Rev Port Cardiol. 2004. PMID: 15478324 English, Portuguese.
-
Head to head comparison of N-terminal pro-B-type natriuretic peptide and B-type natriuretic peptide in patients with/without left ventricular systolic dysfunction.Clin Biochem. 2006 Jun;39(6):640-5. doi: 10.1016/j.clinbiochem.2006.01.021. Epub 2006 Mar 3. Clin Biochem. 2006. PMID: 16516185
-
Diagnostic utility of MR-proANP and NT-proBNP in elderly outpatients with a high risk of heart failure: the Copenhagen heart failure risk study.Biomarkers. 2020 May;25(3):248-259. doi: 10.1080/1354750X.2020.1732466. Epub 2020 Mar 4. Biomarkers. 2020. PMID: 32126847
-
Amino-terminal pro-B-type natriuretic peptide testing for the diagnosis or exclusion of heart failure in patients with acute symptoms.Am J Cardiol. 2008 Feb 4;101(3A):29-38. doi: 10.1016/j.amjcard.2007.11.017. Am J Cardiol. 2008. PMID: 18243855 Review.
-
[Laboratory Aspects of Using the Results of NT-Probnp Concentration Immunochemical Determination in the Management of Patients With Heart Failure: Support For Clinical Decision-Making].Kardiologiia. 2024 Aug 31;64(8):68-78. doi: 10.18087/cardio.2024.8.n2720. Kardiologiia. 2024. PMID: 39262356 Review. Russian.
Cited by
-
N-Terminal Prohormone of Brain Natriuretic Peptide (NT-proBNP) as a Diagnostic Biomarker of Left Ventricular Systolic Dysfunction in Patients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease (AECOPD).Lung. 2018 Oct;196(5):583-590. doi: 10.1007/s00408-018-0137-3. Epub 2018 Jun 27. Lung. 2018. PMID: 29951921
-
B-type natriuretic peptides in chronic obstructive pulmonary disease: a systematic review.BMC Pulm Med. 2017 Jan 10;17(1):11. doi: 10.1186/s12890-016-0345-7. BMC Pulm Med. 2017. PMID: 28073350 Free PMC article.
-
Prognostic implications of heart failure with preserved ejection fraction in patients with an exacerbation of chronic obstructive pulmonary disease.Intern Emerg Med. 2016 Jun;11(4):519-27. doi: 10.1007/s11739-015-1319-0. Epub 2015 Sep 30. Intern Emerg Med. 2016. PMID: 26423072
-
Circulating long non-coding RNAs NRON and MHRT as novel predictive biomarkers of heart failure.J Cell Mol Med. 2017 Sep;21(9):1803-1814. doi: 10.1111/jcmm.13101. Epub 2017 Mar 14. J Cell Mol Med. 2017. PMID: 28296001 Free PMC article.
-
Acute exacerbation of chronic obstructive pulmonary disease: cardiovascular links.Biomed Res Int. 2014;2014:528789. doi: 10.1155/2014/528789. Epub 2014 Mar 2. Biomed Res Int. 2014. PMID: 24724085 Free PMC article. Review.
References
-
- Balter M, Grossman RF (1997) Management of chronic bronchitis and acute exacerbations of chronic bronchitis. Int J Antimicrob Agents 9: 83–93. - PubMed
-
- Balter MS, La Forge J, Low DE, Mandell L, Grossman RF (2003) Canadian guidelines for the management of acute exacerbations of chronic bronchitis: executive summary. Can Respir J 10: 248–258. - PubMed
-
- Donner CF (2006) Acute exacerbation of chronic bronchitis: need for an evidence-based approach. Pulm Pharmacol Ther 19 Suppl 1: 4–10. - PubMed
-
- Sethi S, Muscarella K, Evans N, Klingman KL, Grant BJ, et al. (2000) Airway inflammation and etiology of acute exacerbations of chronic bronchitis. Chest 118: 1557–1565. - PubMed
-
- Sethi S (2000) Infectious etiology of acute exacerbations of chronic bronchitis. Chest 117: 380S–385S. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
