

18-FDG PET/CT assessment of basal cell carcinoma with vismodegib
- PMID: 23342272
- PMCID: PMC3544445
- DOI: 10.1002/cam4.33
18-FDG PET/CT assessment of basal cell carcinoma with vismodegib
Abstract
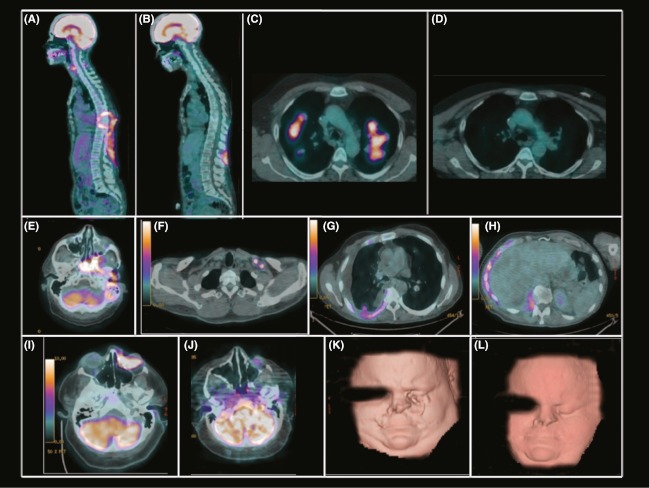
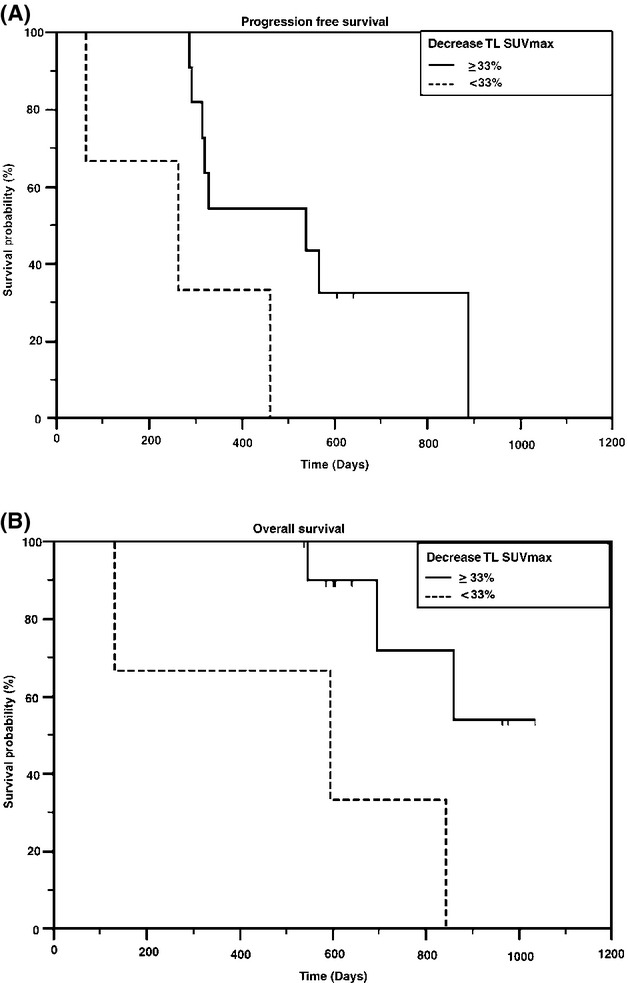
The use of 18-fluorodeoxyglucose (FDG) positron emission tomography with computed tomography (PET/CT) in subjects with advanced basal cell carcinoma (BCC) has not been fully explored due to the rarity of disease presentation. This study evaluated PET/CTs from subjects with advanced BCC participating in a phase I dose-escalation clinical trial of vismodegib. Fourteen subjects with BCC were imaged with 18-FDG PET/CT for lesion identification and response categorizing (European Organisation for Research and Treatment for Cancer [EORTC] and PET response criteria in solid tumors [PERCIST] 1.0). Several parameters including metabolic activity of target lesions, site of disease presentation and spread, treatment response, and prognostic significance of metabolic activity following therapy were evaluated. All subjects exhibited at least one hypermetabolic lesion. Most subjects had only four organ systems involved at study enrollment: skin-muscle (93%), lung (57%), lymph nodes (29%), and bone (21%). SUVmax measured across all lesions decreased (median 33%, SD ± 45%) following therapy with metabolic activity normalizing or disappearing in 42% of lesions. No significant difference was observed between EORTC and PERCIST 1.0. Subjects that demonstrated at least a 33% reduction in SUVmax from baseline had a significantly longer progression-free survival (PFS) (median 17 months, 95% confidence interval [CI] ±4 months vs. 9 months, 95% CI ±5 months, P = 0.038) and overall survival (OS) (median 24 months, 95% CI ±4 months vs. 17 months, 95% CI ±13 months, P = 0.019). BCC lesions are hypermetabolic on 18-FDG PET/CT. A decrease in SUVmax was associated with improved PFS and OS. These results further support the incorporation of 18-FDG PET/CT scans in advanced BCC management.
Trial registration: ClinicalTrials.gov NCT00607724.
Keywords: Basal cell carcinoma; PET/CT; imaging; vismodegib.
Figures
Similar articles
-
Expanded access study of patients with advanced basal cell carcinoma treated with the Hedgehog pathway inhibitor, vismodegib.J Am Acad Dermatol. 2014 Jan;70(1):60-9. doi: 10.1016/j.jaad.2013.09.012. Epub 2013 Nov 1. J Am Acad Dermatol. 2014. PMID: 24189279 Clinical Trial.
-
Comparison of EORTC criteria and PERCIST for PET/CT response evaluation of patients with metastatic colorectal cancer treated with irinotecan and cetuximab.J Nucl Med. 2013 Jul;54(7):1026-31. doi: 10.2967/jnumed.112.111757. Epub 2013 Apr 9. J Nucl Med. 2013. PMID: 23572497 Clinical Trial.
-
Emergence of chemoresistance in a metastatic basal cell carcinoma patient after complete response to hedgehog pathway inhibitor vismodegib (GDC-0449).Australas J Dermatol. 2014 Aug;55(3):218-21. doi: 10.1111/ajd.12196. Australas J Dermatol. 2014. PMID: 25117162
-
A comprehensive review of the role of the hedgehog pathway and vismodegib in the management of basal cell carcinoma.Curr Med Res Opin. 2015 Apr;31(4):743-56. doi: 10.1185/03007995.2015.1018988. Epub 2015 Mar 17. Curr Med Res Opin. 2015. PMID: 25690490 Review.
-
Vismodegib: an inhibitor of the Hedgehog signaling pathway in the treatment of basal cell carcinoma.Ann Pharmacother. 2014 Jan;48(1):99-106. doi: 10.1177/1060028013506696. Epub 2013 Oct 15. Ann Pharmacother. 2014. PMID: 24259609 Review.
Cited by
-
Multimodal imaging of bone metastases: From preclinical to clinical applications.J Orthop Translat. 2015 Aug 13;3(4):166-177. doi: 10.1016/j.jot.2015.07.004. eCollection 2015 Oct. J Orthop Translat. 2015. PMID: 30035055 Free PMC article. Review.
-
Trichoepithelioma Arising in an Ovarian Mature Cystic Teratoma.Case Rep Obstet Gynecol. 2016;2016:6829194. doi: 10.1155/2016/6829194. Epub 2016 Dec 29. Case Rep Obstet Gynecol. 2016. PMID: 28127486 Free PMC article.
-
Comparison of the RECIST and PERCIST criteria in solid tumors: a pooled analysis and review.Oncotarget. 2016 May 10;7(19):27848-54. doi: 10.18632/oncotarget.8425. Oncotarget. 2016. PMID: 27036043 Free PMC article. Review.
-
Advanced basal cell carcinoma, the hedgehog pathway, and treatment options - role of smoothened inhibitors.Biologics. 2015 Nov 6;9:129-40. doi: 10.2147/BTT.S54179. eCollection 2015. Biologics. 2015. PMID: 26604681 Free PMC article. Review.
-
Targeting the Hedgehog Pathway in Cancer: Current Evidence and Future Perspectives.Cells. 2019 Feb 12;8(2):153. doi: 10.3390/cells8020153. Cells. 2019. PMID: 30759860 Free PMC article. Review.
References
-
- Christenson LJ, Borrowman TA, Vachon CM, Tollefson NM, Otley CC, Weaver AL, et al. Incidence of basal cell and squamous cell carcinomas in a population younger than 40 years. JAMA. 2005;294:681–690. - PubMed
-
- Diepgen TL, Mahler V. The epidemiology of skin cancer. Br. J. Dermatol. 2002;146:1–6. - PubMed
-
- Rubin AI, Chen EH, Ratner D. Basal-cell carcinoma. N. Engl. J. Med. 2005;353:2262–2269. - PubMed
-
- Wadhera A, Fazio M, Bricca G, Stanton O. Metastatic basal cell carcinoma: a case report and literature review. How accurate is our incidence data? Dermatol. Online J. 2006;12:7. - PubMed
-
- Hahn H, Wicking C, Zaphiropoulous PG, Gailani MR, Shanley S, Chidambaram A, et al. Mutations of the human homolog of Drosophila patched in the nevoid basal cell carcinoma syndrome. Cell. 1996;85:841–851. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
