

Usefulness of (18)f-fluorodeoxyglucose positron emission tomography/computed tomography in management of cervical dystonia
- PMID: 23342305
- PMCID: PMC3546175
- DOI: 10.5535/arm.2012.36.6.745
Usefulness of (18)f-fluorodeoxyglucose positron emission tomography/computed tomography in management of cervical dystonia
Abstract
Objective: To evaluate the usefulness of (18)F-fluorodeoxyglucose positron emission tomography/computed tomography ((18)F-FDG PET/CT) in the management of cervical dystonia (CD) with botulinum toxin type A (BoNT-A) injection.
Method: Thirty two subjects with CD were included. A BoNT-A injection was provided either by clinically targeting method (group 1) or by (18)F-FDG PET/CT-assisted, clinically targeting method (group 2). In group 2, selection of target muscles and dosage of BoNT-A were determined according to the increased (18)F-FDG uptake, in addition to physical examination and functional anatomy. The outcomes of BoNT-A injection was compared between the two groups, in terms of the number of subjects who had reinjection before and after 6 months, the number of reinjections, the interval of reinjections, the duration to the minimal Toronto Western Spasmodic Torticollis Rating Scale (TWSTRS), the number of adverse events, the reduction rate of TWSTRS at 1-3 months and 3-6 months after injection, and the probability of reinjection-free living.
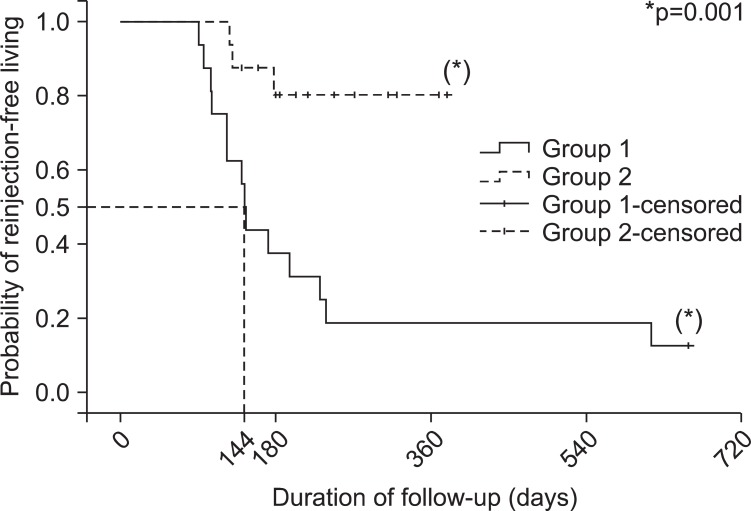
Results: The number of subjects who had reinjection within 6 months was significantly lower in group 2 than in group 1 (10 in group 1 vs. 3 in group 2). The reduction rate of TWSTRS after 3-6 months (37.8±15.7% of group 1 vs. 63.3±28.0% of group 2) and the probability of reinjection-free living were significantly higher in group 2 than in group 1.
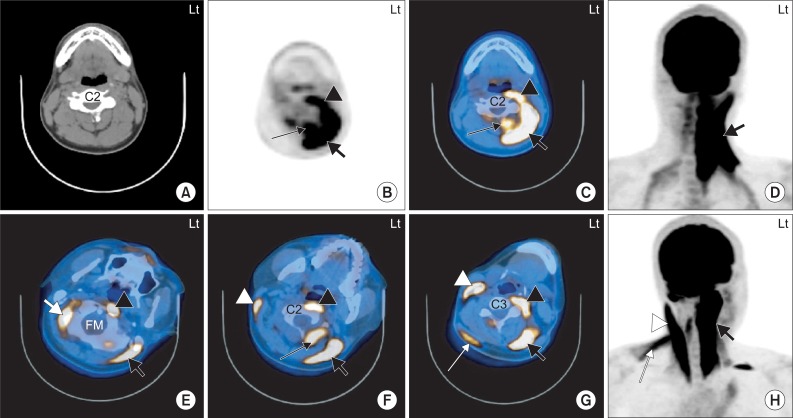
Conclusion: These findings suggest that (18)F-FDG PET/CT study could be useful in management of CD in terms of the identification of dystonic muscles if there is an increase in the (18)F-FDG uptake in the cervical muscle of the images.
Keywords: 18F-Fluorodeoxyglucose; Botulinum toxin; Cervical dystonia; Positron emission tomography.
Figures
References
-
- Jankovic J, Leder S, Warner D, Schwartz K. Cervical dystonia: clinical findings and associated movement disorders. Neurology. 1991;41:1088–1091. - PubMed
-
- Dauer WT, Burke RE, Greene P, Fahn S. Current concepts on the clinical features, aetiology and management of idiopathic cervical dystonia. Brain. 1998;121:547–560. - PubMed
-
- Jankovic J. Treatment of cervical dystonia with botulinum toxin. Mov Disord. 2004;19(Suppl 8):S109–S115. - PubMed
-
- Jankovic J, Tsui J, Bergeron C. Prevalence of cervical dystonia and spasmodic torticollis in the United States general population. Parkinsonism Relat Disord. 2007;13:411–416. - PubMed
-
- Nutt JG, Muenter MD, Aronson A, Kurland LT, Melton LJ., 3rd Epidemiology of focal and generalized dystonia in Rochester, Minnesota. Mov Disord. 1988;3:188–194. - PubMed
LinkOut - more resources
Full Text Sources
