

doi: 10.3201/eid1902.120039.
Eastern equine encephalitis in children, Massachusetts and New Hampshire,USA, 1970-2010
Affiliations
- PMID: 23343480
- PMCID: PMC3559032
- DOI: 10.3201/eid1902.120039
Item in Clipboard
Eastern equine encephalitis in children, Massachusetts and New Hampshire,USA, 1970-2010
Emerg Infect Dis.
2013 Feb.
Abstract
We describe the clinical, laboratory, and radiographic characteristics of 15 cases of eastern equine encephalitis in children during 1970-2010. The most common clinical and laboratory features were fever, headache, seizures, peripheral leukocytosis, and cerebrospinal fluid neutrophilic pleocytosis. Radiographic lesions were found in the basal ganglia, thalami, and cerebral cortex. Clinical outcomes included severe neurologic deficits in 5 (33%) patients, death of 4 (27%), full recovery of 4 (27%), and mild neurologic deficits in 2 (13%). We identify an association between a short prodrome and an increased risk for death or for severe disease.
Figures
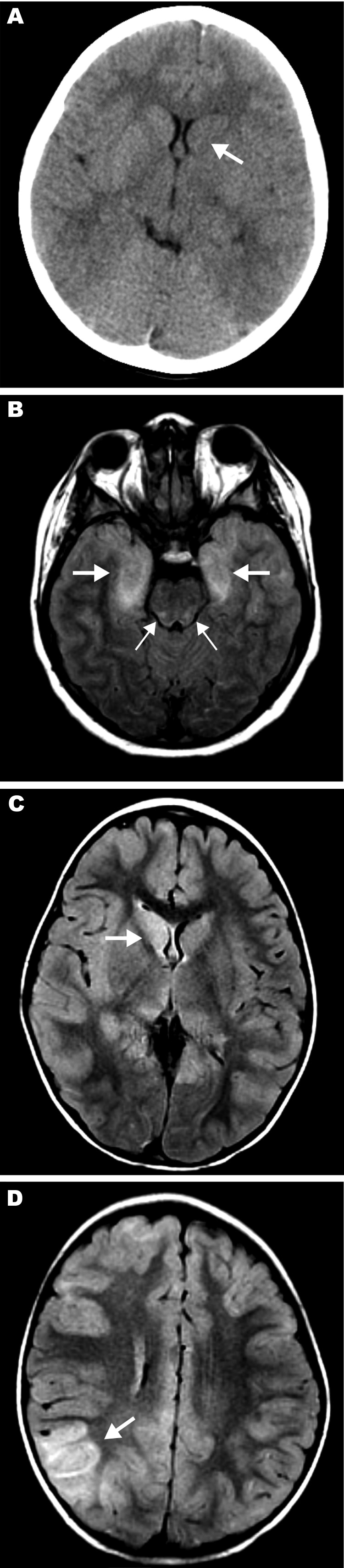
Magnetic resonance images (MRIs) and computed tomography (CT) neuroradiographs showing lesions in brains of 3 children with eastern equine encephalitis A) Results of noncontrast CT scan of the brain of patient 12 on hospital day 2; the neuroradiograph shows subtle hypoattenuation of the left caudate head (arrow) and diencephalic region. B) Axial fluid attenuated inversion recovery (FLAIR) image from brain MRI scan of patient 14 on hospital day 2; the image shows abnormal T2 hyperintense regions of the bimesial temporal regions (thick arrows) with accompanying abnormal T2 hyperintense regions of the dorsal pontomesencephalic regions (thin arrows). C, D) FLAIR images from brain MRI scan of patient 15 on hospital day 3. C) Abnormal T2 hyperintense caudate and thalamic nuclei, most prominent on the right (arrow). D) Abnormal T2 hyperintense regions are most prominent in the right parietotemporal gray matter (arrow) and subcortical white matter but are also seen scattered throughout.
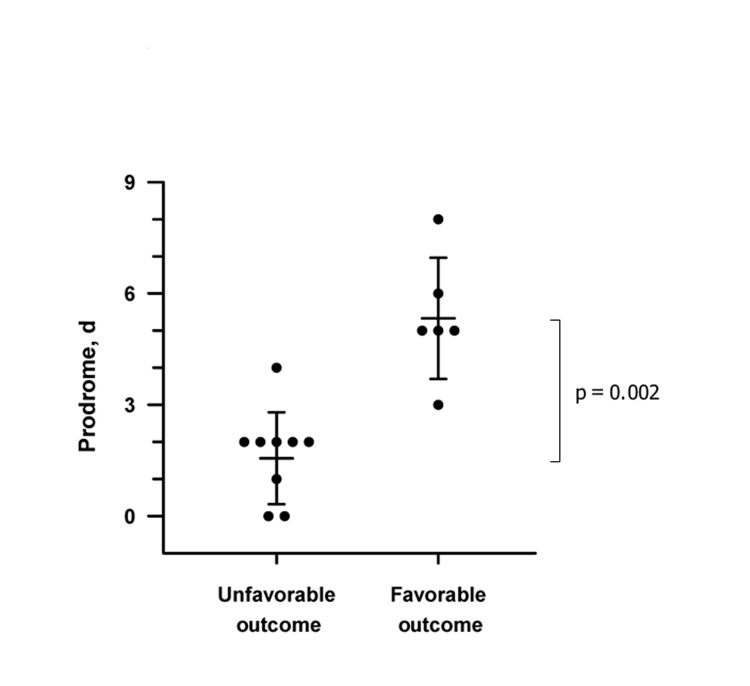
Association of length of prodrome with clinical outcome in children with eastern equine encephalitis. Clinical outcome at the time of hospital discharge was defined by using a modified Pediatric Cerebral Performance Category scale (PCPC) (27). Error bars represent standard deviation; the central lines are the mean. The Mann-Whitney rank-sum test was used to compare the prodrome lengths for patients with favorable outcomes with those for patients with unfavorable outcomes. Prodrome is defined as the time from initial illness symptom to first neurologic symptom. Unfavorable outcome is defined as a PCPC score of 4–6, which includes death and severe neurologic disabilities. Favorable outcome is defined as a PCPC score of 1–3, which includes complete recovery and mild to moderate neurologic disability.
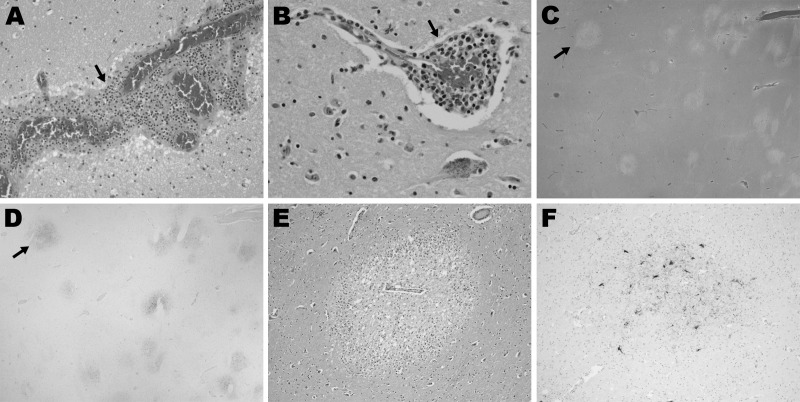
Histopathologic features for patient 12 in a study of children with eastern equine encephalitis (EEE), Massachusetts and New Hampshire, 1970–2010. The postmortem samples of central nervous system tissue were obtained 10 days after the onset of symptoms. A) Hematoxylin and eosin (H&E)–stained section of temporal lobe, showing meningeal inflammation (arrow) (magnification ×200). B) H&E-stained section of midbrain, showing perivascular inflammation (arrow) (magnification ×400). C–F) EEE virus (EEEV) colocalizes with areas of tissue injury in the brain. C) H&E-stained section of the basal ganglia, demonstrating foci of marked tissue rarefaction (arrow) (magnification ×12.5). D) Immunohistochemistry of section adjacent to that shown in panel C; staining of the basal ganglia with EEE immune ascites demonstrates foci of EEEV (arrow) that correspond with areas of tissue rarefaction in panel C (magnification ×12.5). E) H&E-stained section of thalamus (magnification ×100). Specificity for EEEV immunoreactivity of this ascites fluid was confirmed by the lack of staining on control brain specimens (data not shown).
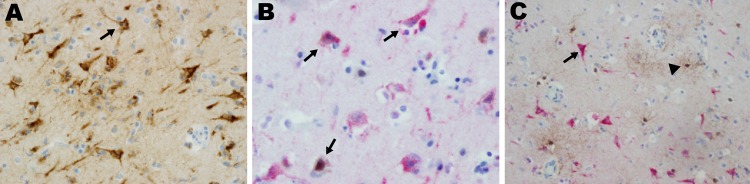
Eastern equine encephalitis virus (EEEV) colocalized with neurons in patient 12 in a study of children with eastern equine encephalitis (EEE), Massachusetts and New Hampshire, 1970–2010. A) Immunohistochemistry, using EEEV immune ascites, of the entorhinal temporal cortex, demonstrating EEEV-infected neurons (arrow) (magnification ×400). B) Dual immunohistochemistry with EEE immune ascites (red stain) and a mouse monoclonal anti–neuronal nuclei (NeuN) antibody (brown stain) demonstrates that EEE-infected cells are NeuN–expressing neurons (arrows) (magnification ×400). C) Dual immunohistochemistry with EEE immune ascites (red stain) and rabbit polyclonal anti-glial fibrillary acidic protein (GFAP) antibody (brown stain) demonstrated that EEE-infected cells (arrow) do not express GFAP and are therefore not glial cells (arrowhead) (magnification ×400). Single antibody immunohistochemistry was performed with heat-induced antigen retrieval, using pressure cooker treatment (120°C for 30 s at 15 psi) with citrate buffer, pH 6.0. Lyophilized ascites from American Type Culture Collection (Manassas, VA, USA) was resuspended in 1 mL of double-distilled H20 and stored as stock solutions at −20°C. The ascites stocks were applied at 1:500 for 40 min at room temperature, after which labeled horseradish peroxidase (HRP) anti-mouse antibody was added, and the stocks were incubated 30 min at room temperature. Visualization was performed by using 3,3′-diaminobenzidine chromogen (Dako EnVision+ System-HRP (DAB); Dakocytomation, Carpinteria, CA, USA). Dual immunohistochemistry was performed by using polyclonal rabbit antibody to GFAP (DAKO, Carpinteria CA, USA) at 1:20,000 and mouse monoclonal anti-NeuN, clone A60, MAB377 (Millipore, Billerica, MA, USA) at 1:7,500. Both antibodies were visualized by using the Dako EnVision+ System-HRP (DAB)-brown, and then EEE immune ascites (1:500) was applied, using the alkaline phosphatase method, and visualized again by using Permanent Red (Dako).
References
-
- Centers for Disease Control and Prevention. Eastern equine encephalitis—New Hampshire and Massachusetts, August–September 2005. MMWR Morb Mortal Wkly Rep. 2006;55:697–700 . - PubMed
-
- Centers for Disease Control and Prevention. Eastern equine encephalitis: epidemiology and geographic distribution [cited 2012 Sept 25]. http://www.cdc.gov/EasternEquineEncephalitis/tech/epi.html#moremapschart...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources