

Unexpected extensions of non-small-cell lung cancer diagnosed during surgery: revisiting exploratory thoracotomies and incomplete resections
- PMID: 23343836
- PMCID: PMC3630409
- DOI: 10.1093/icvts/ivs512
Unexpected extensions of non-small-cell lung cancer diagnosed during surgery: revisiting exploratory thoracotomies and incomplete resections
Abstract
Objectives: Only patients with a complete resection of non-small-cell lung cancer (NSCLC) may expect long-term survival. Despite the recent progress in imaging and induction therapy, a thoracotomy may remain exploratory or with incomplete resection (R2). Our purpose was to revisit these situations.
Methods: A total of 5305 patients who underwent surgery for NSCLC between 1980 and 2009 were reviewed. We compared the epidemiology, pathology, causes and prognosis characteristics of exploratory thoracotomy (ET) and R2 resections.
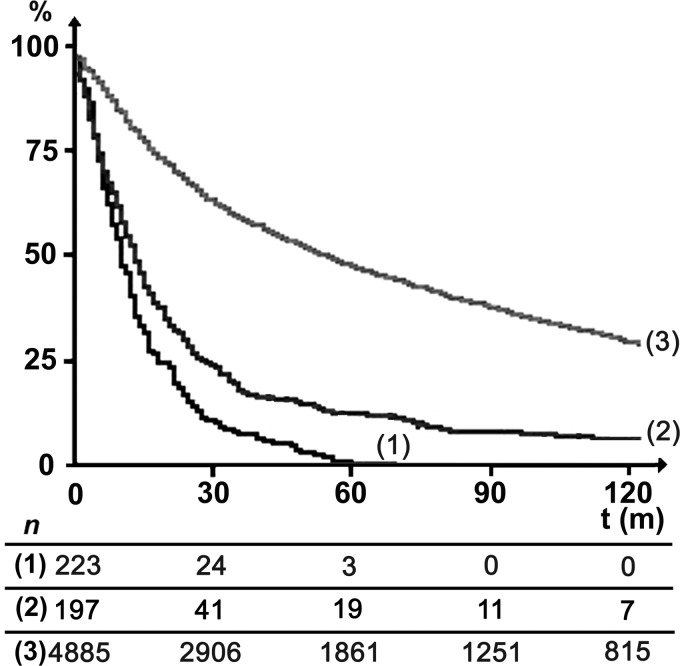
Results: ET and R2 resections were observed in 223 (4%) and 197 (4%) patients, respectively. The frequency of ET decreased with time, while the frequency of R2 resection remained almost stable. The indications for ET and R2 resections were not significantly different. In comparison with ET, R2 resections were characterized by a significantly higher frequency of induction therapy (22 vs 17%, P < 10(-3)), adenocarcinomas (49 vs 15%, P < 10(-6)), T1-T2 (53 vs 29%, P < 10(-6)) and N0-N1 extension (67 vs 42%, P = 10(-6)). R2 resections were also characterized by a higher rate of postoperative complications (19.1 vs 9.9%, P = 0.014), with no significant difference in postoperative mortality (6.9 vs 4.9%, P = non significant). R2 resections resulted in a higher 5-year survival compared with ET (11.1 vs 1.2%, P = 10(-3)). There was no long-term survivor after ET, except during the last decade.
Conclusions: ET and R2 remain unavoidable. In comparison with ET, R2 resection is associated with a higher rate of postoperative complications, but a higher long-term survival.
Figures
Similar articles
-
Is there a survival advantage of incomplete resection of non-small-cell lung cancer that is found to be unresectable at thoracotomy?Interact Cardiovasc Thorac Surg. 2013 Apr;16(4):529-32. doi: 10.1093/icvts/ivs428. Epub 2013 Jan 11. Interact Cardiovasc Thorac Surg. 2013. PMID: 23315183 Free PMC article. Review.
-
No survival benefit of primary tumor resection for non-small cell lung cancer patients with unexpectedly detected pleural disseminated nodules in the era of targeted therapy.Gen Thorac Cardiovasc Surg. 2025 Feb;73(2):102-109. doi: 10.1007/s11748-024-02055-5. Epub 2024 Jul 20. Gen Thorac Cardiovasc Surg. 2025. PMID: 39031333
-
Primary tumour resection showed survival benefits for non-small-cell lung cancers with unexpected malignant pleural dissemination.Interact Cardiovasc Thorac Surg. 2016 Mar;22(3):321-6. doi: 10.1093/icvts/ivv353. Epub 2015 Dec 24. Interact Cardiovasc Thorac Surg. 2016. PMID: 26705302 Free PMC article.
-
Additional pulmonary resections after pneumonectomy: actual long-term survival and functional results.Eur J Cardiothorac Surg. 2008 Sep;34(3):493-8. doi: 10.1016/j.ejcts.2008.05.023. Epub 2008 Jun 25. Eur J Cardiothorac Surg. 2008. PMID: 18583143
-
In lung cancer patients where a malignant pleural effusion is found at operation could resection ever still be justified?Interact Cardiovasc Thorac Surg. 2013 Aug;17(2):407-12. doi: 10.1093/icvts/ivt153. Epub 2013 May 8. Interact Cardiovasc Thorac Surg. 2013. PMID: 23656925 Free PMC article. Review.
Cited by
-
Diagnosis and management of patients with stage III non‑small cell lung cancer: A joint statement by the Lebanese Society of Medical Oncology and the Lebanese Pulmonary Society (Review).Oncol Lett. 2023 Feb 6;25(3):113. doi: 10.3892/ol.2023.13699. eCollection 2023 Mar. Oncol Lett. 2023. PMID: 36844621 Free PMC article. Review.
-
Accidental invisible intrathoracic disseminated pT4-M1a: a distinct lung cancer with favorable prognosis.J Thorac Dis. 2015 Jul;7(7):1205-12. doi: 10.3978/j.issn.2072-1439.2015.05.19. J Thorac Dis. 2015. PMID: 26557992 Free PMC article.
-
Effect of recombinant Newcastle disease virus transfection on lung adenocarcinoma A549 cells in vivo.Oncol Lett. 2014 Dec;8(6):2569-2576. doi: 10.3892/ol.2014.2562. Epub 2014 Sep 25. Oncol Lett. 2014. PMID: 25364430 Free PMC article.
-
Effectiveness of 125I seed implantation in the treatment of non-small cell lung cancer during R2 resection.Oncol Lett. 2017 Dec;14(6):6690-6700. doi: 10.3892/ol.2017.7019. Epub 2017 Sep 21. Oncol Lett. 2017. PMID: 29163696 Free PMC article.
-
Prediction of Pleural Invasion in Challenging Non-Small-Cell Lung Cancer Patients Using Serum and Imaging Markers.Dis Markers. 2020 Feb 7;2020:6430459. doi: 10.1155/2020/6430459. eCollection 2020. Dis Markers. 2020. PMID: 32089756 Free PMC article.
References
-
- American Joint Committee on Cancer (AJCC) AJCC Cancer Staging Manual. In: Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A III, editors. Cancer staging handbook. 7th edn. Chicago: Springer; 2010. pp. 299–323.
-
- van der Drift MA, Karim-Kos HE, Siesling S, Groen HJ, Wouters MW, Coebergh JW, et al. Progress in standard of care therapy and modest survival benefits in the treatment of non-small-cell lung cancer patients in the Netherlands in the last 20 years. J Thorac Oncol. 2012;7:291–8. - PubMed
-
- Oldstraw P, Crowley J, Chansky K, Giroux DJ, Groome PA, Rami-Porta R, et al. The IASLC cancer staging project: proposals for the revision of the TNM Stage Groupings in the forthcoming (seventh) edition of the TNM classification of malignant tumours. J Thorac Oncol. 2007;2:706–14. - PubMed
-
- Mountain CF, Dresler CM. Regional lymph node classification for lung cancer staging. Chest. 1997;111:1718–23. - PubMed
-
- Kwiatkowski F. SEM (Statistiques, Epidémiologie, Médecine): un outil de gestion informatique et statistique adapté à la recherche en cancérologie. Bull Cancer. 2000;87:715–21. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
