

Macrolide-based regimens in absence of bacterial co-infection in critically ill H1N1 patients with primary viral pneumonia
- PMID: 23344833
- PMCID: PMC7094901
- DOI: 10.1007/s00134-013-2829-8
Macrolide-based regimens in absence of bacterial co-infection in critically ill H1N1 patients with primary viral pneumonia
Abstract
Purpose: To determine whether macrolide-based treatment is associated with mortality in critically ill H1N1 patients with primary viral pneumonia.
Methods: Secondary analysis of a prospective, observational, multicenter study conducted across 148 Intensive Care Units (ICU) in Spain.
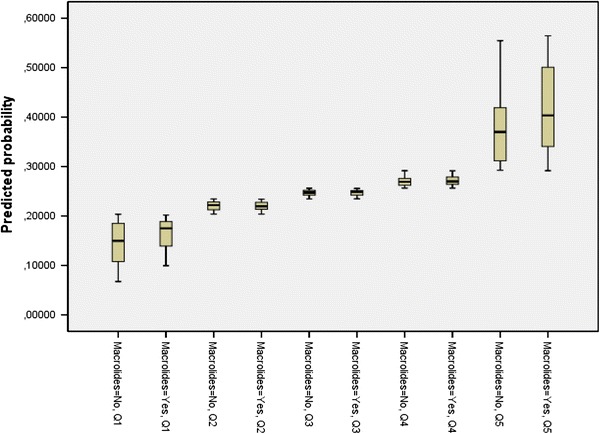
Results: Primary viral pneumonia was present in 733 ICU patients with pandemic influenza A (H1N1) virus infection with severe respiratory failure. Macrolide-based treatment was administered to 190 (25.9 %) patients. Patients who received macrolides had chronic obstructive pulmonary disease more often, lower severity on admission (APACHE II score on ICU admission (13.1 ± 6.8 vs. 14.4 ± 7.4 points, p < 0.05), and multiple organ dysfunction syndrome less often (23.4 vs. 30.1 %, p < 0.05). Length of ICU stay in survivors was not significantly different in patients who received macrolides compared to patients who did not (10 (IQR 4-20) vs. 10 (IQR 5-20), p = 0.9). ICU mortality was 24.1 % (n = 177). Patients with macrolide-based treatment had lower ICU mortality in the univariate analysis (19.2 vs. 28.1 %, p = 0.02); however, a propensity score analysis showed no effect of macrolide-based treatment on ICU mortality (OR = 0.87; 95 % CI 0.55-1.37, p = 0.5). Moreover, the sensitivity analysis revealed very similar results (OR = 0.91; 95 % CI 0.58-1.44, p = 0.7). A separate analysis of patients under mechanical ventilation yielded similar results (OR = 0.77; 95 % CI 0.44-1.35, p = 0.4).
Conclusion: Our results suggest that macrolide-based treatment was not associated with improved survival in critically ill H1N1 patients with primary viral pneumonia.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
