

Sedation depth and long-term mortality in mechanically ventilated critically ill adults: a prospective longitudinal multicentre cohort study
- PMID: 23344834
- PMCID: PMC3625407
- DOI: 10.1007/s00134-013-2830-2
Sedation depth and long-term mortality in mechanically ventilated critically ill adults: a prospective longitudinal multicentre cohort study
Abstract
Purpose: To ascertain the relationship among early (first 48 h) deep sedation, time to extubation, delirium and long-term mortality.
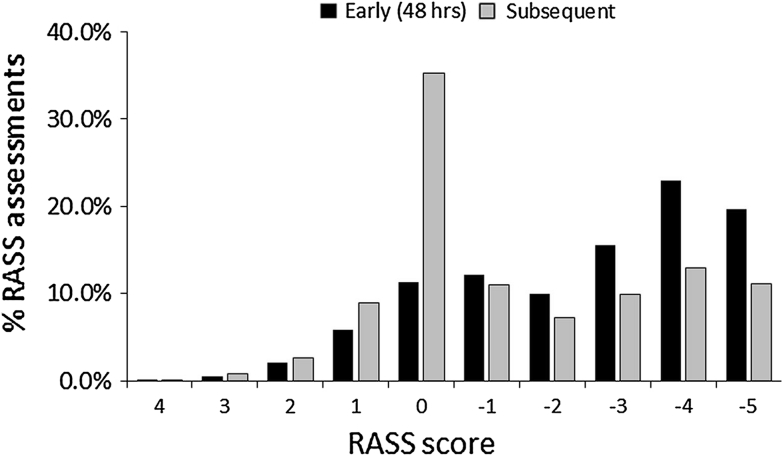
Methods: We conducted a multicentre prospective longitudinal cohort study in 11 Malaysian hospitals including medical/surgical patients (n = 259) who were sedated and ventilated ≥24 h. Patients were followed from ICU admission up to 28 days in ICU with 4-hourly sedation and daily delirium assessments and 180-day mortality. Deep sedation was defined as Richmond Agitation Sedation Score (RASS) ≤-3.
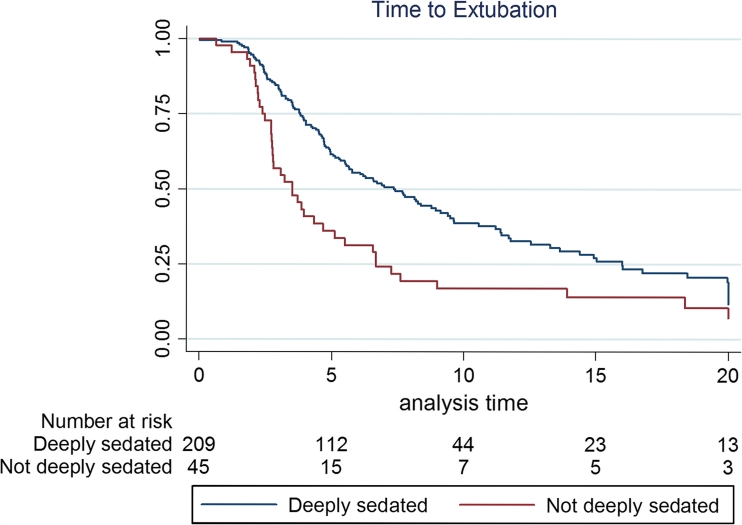
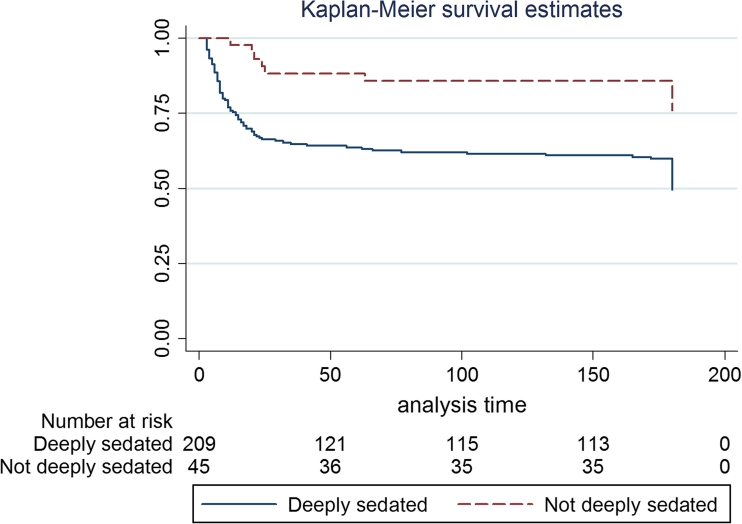
Results: The cohort had a mean (SD) age of 53.1 (15.9) years and APACHE II score of 21.3 (8.2) with hospital and 180-day mortality of 82 (31.7%) and 110/237 (46.4%). Patients were followed for 2,657 ICU days and underwent 13,836 RASS assessments. Midazolam prescription was predominant compared to propofol, given to 241 (93%) versus 72 (28%) patients (P < 0.0001) for 966 (39.6%) versus 183 (7.5%) study days respectively. Deep sedation occurred in (182/257) 71% patients at first assessment and in 159 (61%) patients and 1,658 (59%) of all RASS assessments at 48 h. Multivariable Cox proportional hazard regression analysis adjusting for a priori assigned covariates including sedative agents, diagnosis, age, APACHE II score, operative, elective, vasopressors and dialysis showed that early deep sedation was independently associated with longer time to extubation [hazard ratio (HR) 0.93, 95% confidence interval (CI) 0.89-0.97, P = 0.003], hospital death (HR 1.11, 95% CI 1.05-1.18, P < 0.001) and 180-day mortality (HR 1.09, 95% CI 1.04-1.15, P = 0.002), but not time to delirium (HR 0.98, P = 0.23). Delirium occurred in 114 (44%) of patients.
Conclusion: Irrespective of sedative choice, early deep sedation was independently associated with delayed extubation and higher mortality, and thus was a potentially modifiable risk in interventional trials.
Figures
References
-
- Jacobi J, Fraser GL, Coursin DB, et al. Clinical practice guidelines for sustained use of sedatives and analgesics in the critically ill adults: Task Force of the American College of Critically Care Medicine (ACCM) of Society of Critical Care Medicine (SCCM), American Society of Health-System Pharmacists (ASHP), American College of Chest Physicians. Crit Care Med. 2002;30:119–141. doi: 10.1097/00003246-200201000-00020. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
